

-

-
---------
-
"Health Care Reform for Beginners"
-
http://voices.washingtonpost.com/ezra-klein/2009/06/health_care_reform_for_beginne_3.html?hpid=topnews
-
-----
-
INTERACTIVE: In Search of Health-Care Reform
-
www.washingtonpost.com/wp-srv/package/health-care-reform09/index.html
-
---------
Source: Paul Krugman, "Voodoo Health Economics", NY Times, Op-Ed, 4/4/2008
American healthcare insurance companies hold down costs by only covering healthy people, denying as many claims as possible, & forcing doctors & hospitals to spend money in litigation to get paid.
The United States has the most privatized healthcare insurance system, with the most market competition - and it has the highest healthcare costs in the World.
Privatization equals: High costs per person covered.
My analysis (by Jonathan Melle): The system incentivizes healthy adults to subscribe to private health insurance. Once a subscriber becomes ill, there is a gap in health coverage due to A PRE-EXISTING CONDITION. The system is reactive & does not prioritize preventive care. Until one is disabled, one is without comprehensive care.
Source: Paul Krugman, "Voodoo Health Economics", NY Times, Op-Ed, 4/4/2008
---------
News Article:
From the Los Angeles Times
Health Insurer Tied Bonuses To Dropping Sick Policyholders
Lisa Girion
Los Angeles Times Staff Writer
November 9, 2007
One of the state's largest health insurers set goals and paid bonuses based in part on how many individual policyholders were dropped and how much money was saved.
Woodland Hills-based Health Net Inc. avoided paying $35.5 million in medical expenses by rescinding about 1,600 policies between 2000 and 2006. During that period, it paid its senior analyst in charge of cancellations more than $20,000 in bonuses based in part on her meeting or exceeding annual targets for revoking policies, documents disclosed Thursday showed.
The revelation that the health plan had cancellation goals and bonuses comes amid a storm of controversy over the industry-wide but long-hidden practice of rescinding coverage after expensive medical treatments have been authorized.
These cancellations have been the recent focus of intense scrutiny by lawmakers, state regulators and consumer advocates. Although these "rescissions" are only a small portion of the companies' overall business, they typically leave sick patients with crushing medical bills and no way to obtain needed treatment.
Most of the state's major insurers have cancellation departments or individuals assigned to review coverage applications. They typically pull a policyholder's records after major medical claims are made to ensure that the client qualified for coverage at the outset.
The companies' internal procedures for reviewing and canceling coverage have not been publicly disclosed. Health Net's disclosures Thursday provided an unprecedented peek at a company's internal operations and marked the first time an insurer had revealed how it linked cancellations to employee performance goals and to its bottom line.
The bonuses were disclosed at an arbitration hearing in a lawsuit brought by Patsy Bates, a Gardena hairdresser whose coverage was rescinded by Health Net in the middle of chemotherapy treatments for breast cancer. She is seeking $6 million in compensation, plus damages.
Insurers maintain that cancellations are necessary to root out fraud and keep premiums affordable. Individual coverage is issued to only the healthiest applicants, who must disclose preexisting conditions.
Other suits have been settled out of court or through arbitration, out of public view. Until now, none had gone to a public trial.
Health Net had sought to keep the documents secret even after it was forced to produce them for the hearing, arguing that they contained proprietary information and could embarrass the company. But the arbitrator in the case, former Los Angeles County Superior Court Judge Sam Cianchetti, granted a motion by lawyers for The Times, opening the hearing to reporters and making public all documents produced for it.
At a hearing on the motion, the judge said, "This clearly involves very significant public interest, and my view is the arbitration proceedings should not be confidential."
The documents show that in 2002, the company's goal for Barbara Fowler, Health Net's senior analyst in charge of rescission reviews, was 15 cancellations a month. She exceeded that, rescinding 275 policies that year -- a monthly average of 22.9.
More recently, her goals were expressed in financial terms. Her supervisor described 2003 as a "banner year" for Fowler because the company avoided about "$6 million in unnecessary health care expenses" through her rescission of 301 policies -- one more than her performance goal.
In 2005, her goal was to save Health Net at least $6.5 million. Through nearly 300 rescissions, Fowler ended up saving an estimated $7 million, prompting her supervisor to write: "Barbara's successful execution of her job responsibilities have been vital to the profitability" of individual and family policies.
State law forbids insurance companies from tying any compensation for claims reviewers to their claims decisions.
But Health Net's lawyer, William Helvestine, told the arbitrator in his opening argument Thursday that the law did not apply to the insurer in the case because Fowler was an underwriter -- not a claims reviewer.
Helvestine acknowledged that the company tied some of Fowler's compensation to policy cancellations, including Bates'. But he maintained that the bonuses were based on the overall performance of Fowler and the company. He also said that meeting the cancellation target was only a small factor.
The documents showed that Fowler's annual bonuses ranged from $1,654 to $6,310. But Helvestine said that no more than $276 in any year was connected to cancellations.
He said Fowler's supervisor, Mark Ludwig, set goals that were reasonable based on the prior year's experience.
"I think it is insulting to those individuals to make this the focal point of this case," Helvestine said.
Bates' lawyer, William Shernoff, said Health Net's behavior was "reprehensible."
He said the cancellation goals and financial rewards showed that the company canceled policies in bad faith and just to save money. After all, he told the arbitrator, canceling policies was Fowler's primary job.
"For management to set goals in advance to achieve a certain number of rescissions and target savings in the millions of dollars at the expense of seriously ill patients is cruel and reprehensible by any standards of law or decency," Shernoff said.
The company declined requests to make Fowler available to discuss the reviews.
Cianchetti, the arbitrator, earlier ruled the rescission invalid because Health Net had mishandled the way it sent Bates the policy when it issued coverage. At the end of the hearing, it will be up to Cianchetti to determine whether Health Net acted in bad faith and owes Bates any damages.
The disclosures surprised regulators. A spokesman said state Insurance Commissioner Steve Poizner was troubled by the allegations.
"Commissioner Poizner has made it clear he will not tolerate illegal rescissions," spokesman Byron Tucker said. "We are going to take a hard and close look at this case."
In recent months, the state's health and insurance regulators have teamed to develop rules aimed at curbing rescissions and to more closely monitor the industry's cancellation policies.
Other insurers that have rescission operations, including Blue Cross of California and Blue Shield of California, said they had no similar policies linking employee performance reviews to rescission levels. Blue Cross said it conducted audits to ensure that claims reviewers were not given any "carrots" for canceling coverage.
Bates, who filed the suit against Health Net, owns a hair salon in a Gardena mini-mall between a liquor store and a doughnut shop. She said she was left with nearly $200,000 in medical bills and stranded in the midst of chemotherapy when Health Net canceled her coverage in January 2004.
Bates, 51, said the first notice she had that something was awry with her coverage came while she was in the hospital preparing for lump-removal surgery.
She said an administrator came to her room and told her the surgery, scheduled for early the next day, had been canceled because the hospital learned she had insurance problems. Health Net allowed the surgery to go forward only after Bates' daughter authorized the insurance company to charge three months of premiums in advance to her debit card, Bates alleged. Her coverage was canceled after she began post-surgical chemotherapy threatments.
"I've got cancer, and I could die," she said in a recent interview. Health Net "walked away from the agreement. They don't care."
Health Net contended that Bates failed to disclose a heart problem and shaved about 35 pounds off her weight on her application. Had it known her true weight or that she had been screened for a heart condition related to her use of the diet drug combination known as fen-phen, it would not have covered her in the first place, the company said.
"The case was rescinded based on inaccurate information on the individual's application," Health Net spokesman Brad Kieffer said.
Bates said she already had insurance when a broker came by her shop in the summer of 2003, and said she now regretted letting him in the door. She agreed to apply to Health Net when the broker told her he could save her money, Bates said.
She added that she never intended to mislead the company. Bates said the broker filled out the application, asking questions about her medical history as she styled a client's hair in her busy shop and he talked to another client waiting for an appointment at the counter. She maintained that she answered his questions as best she could and did not know whether he asked every question on the application.
Bates' chemotherapy was delayed for four months until it was funded through a program for charity cases. Three years later, she can't afford the tests she needs to determine whether the cancer is gone.
So she is left to worry. She is also left with a catheter embedded in her chest where the chemotherapy drugs were injected into her bloodstream. Bates said she found a physician willing to remove it without charge, but he won't do it without a clear prognosis. That remains uncertain.
Shernoff, Bates' lawyer, claimed that the performance goals for Fowler showed that Health Net was bent on finding any excuse to cancel the coverage of people like Bates to save money.
"I haven't seen this kind of thing for years," Shernoff said. "It doesn't get much worse."
----------
Maine: Pat LaMarche 2006

----------




----------
US among worst in world for infant death, By The Associated Press, 11/11/2007
The rate at which infants die in the United States has dropped substantially over the past half-century, but broad disparities remain among racial groups, and the country stacks up poorly next to other industrialized nations.
In 2004, the most recent year for which statistics are available, roughly seven babies died for every 1,000 live births before reaching their first birthday, the Centers for Disease Control and Prevention says. That was down from about 26 in 1960.
Babies born to black mothers died at two and a half times the rate of those born to white mothers, according to the CDC figures.
The United States ranks near the bottom for infant survival rates among modernized nations. A Save the Children report last year placed the United States ahead of only Latvia, and tied with Hungary, Malta, Poland and Slovakia.
The same report noted the United States had more neonatologists and newborn intensive care beds per person than Australia, Canada and the United Kingdom — but still had a higher rate of infant mortality than any of those nations.
Doctors and analysts blame broad disparities in access to health care among racial and income groups in the United States.
Not surprisingly, the picture is far bleaker in poorer countries, particularly in Africa. A 2005 World Health Organization report found infant mortality rates as high as 144 per 1,000 births — more than 20 times the U.S. rate — in Liberia.
-

ADVANCE FOR NOV. 11; graphic shows 2006 infant mortality in Tennessee by county and annual numbers by race for Shelby County and state since 1990
----------
Op-Ed, RACHEL NARDIN, The Boston Globe
Healthcare for vets - and all others
By Rachel Nardin | November 11, 2007
EVEN AS our government puts members of our armed services in harm's way, it is failing to care for them once they return home. Soldiers get excellent acute care when injured on active duty, but as revelations of poor conditions for soldiers receiving ongoing outpatient care at the Walter Reed Army Medical Center highlighted, service members often have trouble getting the care they need once active duty ends.
According to a study by some of my colleagues at Harvard Medical School, to be published in next month's American Journal of Public Health, nearly 1.8 million veterans had no health insurance in 2004, up 290,000 since 2000. An additional 3.8 million members of their households were also uninsured and ineligible for care at hospitals and clinics run by the Veterans Health Administration of the Department of Veterans Affairs. The 2006 data released this year show little change in these numbers.
Many uninsured veterans are barred from VA care because of a 2003 Bush administration order that halted enrollment of most middle-income veterans. Others are unable to obtain VA care because of unaffordable copayments for VA specialty care, waiting lists at some facilities or the lack of VA facilities in their communities. Almost two-thirds of uninsured veterans were employed, and nearly 9 out of 10 had worked within the past year. Most uninsured veterans were in working families. Many earned too little to afford health insurance, but too much to qualify for free care under Medicaid or VA rules.
The VA is a rare success story in our healthcare system. The system offers more equitable and higher quality care than the average care in the private sector, and has become a medical leader in research, primary care, and computerization. Studies in the Annals of Internal Medicine and elsewhere have shown that compared with patients in HMOs, a higher percentage of patients at VA facilities have adequate control of high blood pressure and diabetes, and receive appropriate medications after a heart attack. So it's not the quality of care that veterans receive that's the problem; rather, it's their restricted access to care.
What can we do to ensure that all our veterans have access to affordable, high-quality healthcare? In the short term the government can roll back the income restrictions on VA care. However, this would still leave many veterans unable to access care because they live far from VA facilities. Moreover, even complete coverage of veterans would leave 3.8 million of their family members uninsured. In this regard, these families are in the same position as civilian families who cannot get care because they are uninsured, are denied care by their insurance companies or can't afford the necessary copays and deductibles.
In the long term, the difficulty returning veterans have in obtaining healthcare cannot be solved on its own. Across the health field, costs are spiraling. Payers, whether the government or private insurers, are trying to stay within budget by offering less care, offering care to fewer people or shifting costs of care to patients. If we do nothing, there's no improvement in sight.
The problems with veterans' healthcare offer further evidence of why the US healthcare system needs to be reformed. Because we pay for healthcare through a patchwork of private insurance companies, nearly one-third of our health spending goes to administration. Replacing private insurers with national health insurance would recover money currently squandered on billing, marketing, underwriting, and other activities. Eliminating this waste has been estimated to save $350 billion per year. Combined with what we're already spending, this is enough to provide comprehensive coverage for everyone.
With a national health insurance program, all veterans who desired could continue to receive care at VA facilities, or they could choose to receive care in the private sector. None of our veterans, or their families, would fall through the cracks.
Ultimately, only active government intervention can guarantee that veterans have the healthcare they need. They and their families - and, in fact, all Americans - deserve equal access to high-quality, affordable healthcare.
Dr. Rachel Nardin is assistant professor of neurology at Harvard Medical School.
----------
News Article:
The Berkshire Eagle Online -
Health Care Plan could need $146M
As many as 180,000 people could be enrolled by the end of June, which could result in a shortage in program funding
Wire and staff reports
Monday, November 19, 2007
BOSTON — Those working to promote Massachusetts' new health care law have been so successful in enrolling people in subsidized health plans that the state may need millions more to pay for the program.
An outreach effort by local advocates, state health officials and hospitals has put Massachusetts on the path to enrolling as many as 180,000 people by the end of June.
That could put the program short by about $146 million. The state set aside $472 million this fiscal year for the subsidized program, based on estimates on the number of people who would enroll.
Supporters of the law say they are pleased that more people are being insured but concerned about how the state will find the money to close the gap.
"It's less a health care challenge and more a budget challenge," said state Sen. Benjamin B. Downing, D-Pittsfield.
"The next step now is dealing with health care costs," he said.
Despite the challenges, "it's not necessarily a negative thing that more people are enrolled," Downing said.
Some of his Senate colleagues agree with that sentiment.
"It's a good problem to have. People are getting insured and, hopefully, getting care," state Sen. Richard Moore, D-Uxbridge, told the Boston Sunday Globe.
But Moore, who is co-chairman of the Legislature's Health Care Financing Committee, also sounded a note of caution, saying, "Any shortfall is a big deal."
Not everyone is convinced that the state will fall as far short as predicted, saying the projections may be too high because there is little precedent for the landmark law, which requires nearly everyone in Massachusetts to be insured or face increasing tax penalties.
But if the state needs more money to pay those extra insurance bills, it could look to a limited number of options.
Lawmakers could appropriate more money from the state budget or cut extra payments to certain hospitals that were included in the law mandating coverage.
One thing the state isn't considering is blocking anyone eligible for subsidized care from obtaining it, according to Gov. Deval L. Patrick's top budget chief Leslie Kirwan, who also chairs the board overseeing the health care law.
"It's too early to make any departure from the health reform plan," Kirwan said. "We'll follow the trends and adjust, if needed."
The state program, called Commonwealth Care, provides subsidized care to anyone earning between the federal poverty level and three times that amount or about $31,000 for an individual. How much a person contributes to the premiums increases depending on their income.
Anyone making less than the federal poverty level is entitled to virtually free care. Those making more than three times the level must obtain nonstate-subsidized health insurance.
Pressure could increase at the start of the new fiscal year on July 1. That's when insurers who participate in the subsidized program are expected to ask for increased payments from the state.
Observers credit the spike in the number of people enrolling for subsidized health care on a coordinated public education push by the state, hospitals, community outreach workers and insurers.
John McDonough, executive director of the advocacy group Health Care for All, called the increased numbers a sign of success.
"The sky is not falling," he said. "There is a budget challenge."
Berkshire Eagle reporter Conor Berry contributed to this report.
----------
The Boston Globe - Letters:
Blue Cross CEO's pay out of line
November 19, 2007
RE "BLUE Cross gave chairman $16.4m in retirement pay: Van Faasen still on salary at insurer" (Business, Nov. 16): At a time when the cost of health insurance and the numbers of uninsured are rising, all sectors of the healthcare community must exercise prudent management of every healthcare dollar. This responsibility cannot be borne solely by the provider sector while the insurance industry passes expenses on to subscribers and employers.
Blue Cross and Blue Shield of Massachusetts voted its CEO a total of $19.4 million in salary and benefits while retaining him as chairman. Because Blue Cross-Blue Shield is a not-for-profit entity, Massachusetts considers it a public charity. As such, the insurer, its board of directors, and the state officials charged with the oversight of public charities should be held accountable by the citizens of the state for better guardianship of the public trust.
Dr. GERALD B. HEALY
Chicago
The writer is president of the American College of Surgeons.
--
THE BOSTON GLOBE
Blue Cross gave chairman $16.4m in retirement pay
Van Faasen still on salary at insurer
By Jeffrey Krasner, Globe Staff | November 16, 2007
William C. Van Faasen, the long-time chairman and chief executive of Blue Cross and Blue Shield of Massachusetts, was paid $16.4 million in retirement benefits in January 2006, even though he didn't leave the company.
The payment was triggered when Van Faasen, 58, stepped down as chief executive, retaining his position as chairman of the state's largest health insurer with 3 million members. In addition to the retirement payout, he also earned nearly $3 million last year in salary and bonus as chairman.
Van Faasen is credited with engineering much of the insurer's success over the last 15 years. But the size of his retirement benefit at a nonprofit, and the conditions under which it was awarded, raised questions and concerns yesterday.
"When you're spending down the coffers by paying $19 million to reward a CEO for changing jobs, premiums are going to have to increase," said Jerry Flanagan, healthcare policy director for the Foundation for Taxpayer and Consumer Rights, a nonprofit, nonpartisan consumer group in Los Angeles. "Double-digit premium increases that are fueled by insurance company excesses like this are uninsuring the insured."
State Senator Mark C. Montigny, Democrat of New Bedford, said, "Bill Van Faasen is a good guy and he's done a great job, but if he wants that kind of money, he should run a hedge fund."
Van Faasen was recruited from Michigan Blue Cross in 1990, and was named chief executive in 1992. He was named chairman in 2002. In mid-2005, Cleve L. Killingsworth Jr. succeeded him as chief executive. Since then, Van Faasen has served only as chairman. In September, Blue Cross said he would retire and leave the company at year-end.
Blue Cross's 2006 executive pay was disclosed yesterday in filings to the attorney general. Van Faasen earned a salary of $500,000 and a performance-based bonus of $2.46 million. Killingsworth earned a salary of $903,000 and bonus of $1.36 million. Chris Murphy, a spokesman for Blue Cross Blue Shield of Massachusetts, said Van Faasen's salary and retirement contributions were evaluated by external compensation consultants, who assured the company the payments "met industry standards."
"The board meets annually and discusses CEO compensation," said Murphy. "This is a large amount of compensation, and it reflects his extraordinary performance as chief executive of Blue Cross Blue Shield of Massachusetts."
Senior executives of large companies often put aside some of their pay into a separate account, where it can grow before it is paid out. But none of the money paid to Van Faasen consisted of so-called deferred compensation.
"The $16.4 million is based on his tenure here and the performance of the company," said Murphy.
Only $5.5 million of the retirement payment was previously reported in filings with the state. The balance wasn't previously reported, Murphy said, because the money didn't technically belong to Van Faasen until he received it, and state rules did not require that portion of the payment to be disclosed in annual reports. In addition, he said, the actual amount could not be determined until his retirement date was set.
Linda Crompton, chief executive of BoardSource, a Washington organization that advises nonprofits about board and corporate oversight issues, questioned the size of Van Faasen's payment because Blue Cross is a nonprofit exempt from paying income taxes.
"Would this payment meet the standards of reasonable behavior?" she asked. "I don't know. It seems like a large sum of money."
In addition, Crompton criticized Blue Cross's succession planning, in which Van Faasen gave up the chief executive position, but retained his seat as chairman.
"That's definitely a poor practice," she said. "If someone is officially retired, good practice is they leave the organization. They shouldn't move into another role where they continue to take money from the company. The positions are supposed to be independent."
In May 2005, Van Faasen told the Globe he was stepping down as chief executive because he had achieved his goals. He said he came to the insurer to "turn around a company and restore its confidence and connection to the community."
Other health insurers also disclosed executive compensation yesterday. In 2006, Harvard Pilgrim Health Care, the state's second-largest health insurer, paid chief executive Charles D. Baker $1.5 million in salary and bonus. James Roosevelt Jr., chief executive of Tufts Health Plan, earned nearly $1.3 million including contributions to benefit plans.
The health plans also reported financial results for the third quarter of 2007. Blue Cross Blue Shield of Massachusetts earned $110 million, with strong increases in operating income and investment income compared to the same period a year ago. Harvard Pilgrim reported net income of $20.4 million, down slightly from $21.4 million in last year's third quarter. Revenue was also down slightly, from $640 million to $631.9 million.
Tufts Health Plan reported net income of $41 million. Results were boosted by nearly $17.3 million in investment income. Membership reached 654,000 in September, an increase of about 50,000 since January.
Jeffrey Krasner can be reached at krasner@globe.com.
-----
"Mass. panel approves changes to subsidized residents health plan"
By Alice Dembner, Boston Globe Staff | December 14, 2007
Striving to hold down costs to taxpayers, a state panel yesterday approved a range of changes for next year for the rapidly growing subsidized health insurance program. The changes will probably cut payments to doctors and hospitals, reduce choices for patients, and possibly increase how much patients have to pay.
The program is the centerpiece of the state's landmark effort to insure nearly every resident, and there is widespread concern about long-term funding of the initiative because of growing healthcare costs.
In the first year, the program for low-income people has enrolled nearly 160,000, far more than anticipated, and state officials have estimated that the cost could run as high as $619 million for the current fiscal year, $147 million over budget.
State officials yesterday declined to offer predictions of next year's costs, but said they were trying to keep the program affordable for the state and enrollees.
The goal "is to make this great healthcare reform effort sustainable," said Leslie Kirwan, secretary of administration and finance and chairwoman of the Commonwealth Health Insurance Connector Authority, which is overseeing the insurance initiative.
The authority's board agreed yesterday on bid specifications for insurers that would use multiple means to reduce cost increases and consolidate the program. The vote followed one nine days earlier to press insurers to hold the line on premiums for unsubsidized insurance plans sold through the connector.
For the subsidized plan, called Commonwealth Care, the authority's staff has suggested that costs per member could rise as much as 14 percent next year, if there were no changes.
The bid specifications will direct the four insurers that administer Commonwealth Care to cut payments to healthcare providers by 3 to 5 percent.
"There's no justification to be paying more than Medicaid rates," said Patrick Holland, the authority's chief financial officer.
The board did not consider any reductions in the comprehensive range of services covered by the plan, but decided to push insurers to control spending on patients with substance abuse and chronic conditions through better oversight and follow-up care.
In addition, the board voted to eliminate one part of the program that has been the most expensive per member. That program had allowed patients to pay a higher monthly premium in order to incur lower fees each time they sought care. But the option drew the sickest and oldest patients and was twice as expensive for the state as a plan with lower premiums. The approximately 3,500 patients in that plan will have to shift into an option under which they pay more of the cost per visit.
The connector postponed until February a decision on the most controversial step that would save the state money: increasing copayments and other out-of-pocket costs for tens of thousands of patients with an income above the poverty level.
Commonwealth Care members currently pay much less than those with private insurance to visit a doctor, get prescription drugs, or get hospital care.
Alice Dembner can be reached at Dembner@globe.com.
----------------------------------------
NY-Times: News Article:
----------
Ann F. McEachern, 33, says she will accept the risk and the penalty of being uninsured this year.

Photo by Erik Jacobs for The New York Times
----------
Samuel B. Hagan

He is, 27, who is a courier who also does not have insurance, and he says he is not concerned about serious health problems.
----------
Massachusetts Faces a Test on Health Care
By KEVIN SACK - November 25, 2007
BOSTON, Nov. 20 — As the Democratic presidential candidates debate whether Americans should be forced to obtain health insurance, the people of Massachusetts are living the dilemma in real time.
A year after Massachusetts became the only state to require that individuals have health coverage, residents face deadlines to sign up or lose their personal tax exemption, worth $219 on next year’s state income tax returns. More than 200,000 previously uninsured residents have enrolled, but state officials estimate that at least that number, and perhaps twice as many, have not.
Those managing the enrollment effort say it has exceeded expectations. In particular, state-subsidized insurance packages offered to low-income residents have been so popular that the program’s spending may exceed its budget by nearly $150 million.
But the reluctance of so many to enroll, along with the possible exemption of 60,000 residents who cannot afford premiums, has raised questions about whether even a mandate can guarantee truly universal coverage.
Additional concerns have been generated by projections that the state’s insurers plan to raise rates 10 percent to 12 percent next year, twice this year’s national average. That would undercut the plan’s secondary goal of slowing the increase in health costs.
“We’re going to be very aggressive in trying to get those numbers down to single digits,” said Jon M. Kingsdale, executive director of the Commonwealth Health Insurance Connector Authority, the agency that markets the subsidized insurance policies. “If we continue with double-digit inflation, I don’t think health reform is sustainable.”
The state’s experience should be instructive to the presidential campaigns, and to officials in California, where Gov. Arnold Schwarzenegger, a Republican, has proposed a similar plan. Democratic leaders there initially rejected an individual mandate because labor unions argued that workers might not be able to afford coverage. They have recently reversed course, but have yet to agree with Mr. Schwarzenegger on how to finance the plan.
Each of the three leading contenders for the Democratic presidential nomination has pledged to achieve universal health coverage, which polls show to be a priority for party voters. But as the candidates seek to differentiate themselves, a rift has emerged over whether it is possible to insure all Americans without requiring them to obtain coverage.
Senator Hillary Rodham Clinton of New York and John Edwards, the former North Carolina senator, support a mandate. It is, they say, the only way to guarantee that everyone is covered and to thereby bring down costs by spreading the country’s insurance risk as broadly as possible.
“The sad reality is that the uninsured don’t just struggle with costs themselves, they impose costs on the rest of us,” Mrs. Clinton said in September. “It’s a hidden tax: the high cost of emergency room visits that could have been prevented by a much less expensive doctor’s appointment, the cost of unpaid medical bills that lead insurance companies to raise rates on the rest of us.”
Mr. Edwards echoed those remarks a week later. “The reason the mandate is necessary is because you cannot have universal health care without it,” he said. “Does not exist, and anyone who pretends it is, is not being straight.”
Senator Barack Obama of Illinois sees it a different way. He argues there is danger in mandating coverage before it is clear it can be affordable for those at the margins. While Mr. Obama does not rule out a mandate down the road, his emphasis is on reducing costs and providing generous government subsidies to those who need them. He would mandate coverage for children.
That distinction set off a pointed exchange in the Democratic debate in Las Vegas on Nov. 15. “I don’t think that the problem with the American people is that they are not being forced to get health care,” Mr. Obama said. “The problem is they can’t afford it.”
Mrs. Clinton jabbed back, saying Mr. Obama’s plan “starts from the premise of not reaching universal health care,” a virtual slur in the Democratic campaign. Mr. Obama responded that Mrs. Clinton had yet to explain how she would enforce a mandate. “She is not garnishing people’s wages to make sure that they have it,” he pointed out.
Obama strategists had been considering that point of attack for several weeks. It served the purpose, they said, not only of separating the candidates on a crucial domestic issue, but also of reinforcing their message that Mrs. Clinton does not, in Mr. Obama’s words, provide “straight answers to tough questions.”
Mrs. Clinton discovered the peril of revealing too many policy details in 1993, when the 1,342-page health plan she developed for her husband attracted a legion of opponents. This year, she has said she would leave the particulars of enforcement to her negotiations with Congress.
The Massachusetts plan was signed into law by former Gov. Mitt Romney, who, like each of his rivals for the Republican presidential nomination, does not now support a national insurance mandate. The law, which requires adults to be covered by Dec. 31, grants exemptions from the penalty if an income-based formula determines that coverage would not be affordable.
State officials warned that if policies were not bought this month they were not likely to be in effect by the deadline. But some insurers said they would sell last-minute policies.
The state established a mild penalty for the first year: the loss of the $219 tax exemption. But in the second year, the fine can amount to half the cost of the least expensive policy available, probably at least $1,000.
Ann F. McEachern, 33, a waitress and student who lives in Cambridge, said she did not buy insurance this year but probably would in 2008. “The penalty in 2007 wasn’t enough to kick it up to the top of my priority list,” Ms. McEachern said. “It’s always nice to be insured, but I think I’m at pretty low risk for anything happening to me that would be financially devastating.”
Though officials do not yet have data to determine who the remaining uninsured are, they assume many are in the group they call “the young invincibles.”
“At 27, it’s not like I’m thinking, ‘Oh, man, what if I need an operation down the line?’ ” said Samuel B. Hagan of Lenox, a courier who remains uninsured. “Furthest thing from my head.”
John E. McDonough, executive director of Health Care for All, an advocacy group based here, said he found it breathtaking that political leaders were calling for an individual mandate well before there was any way to measure the success of the Massachusetts experiment.
But Diane Rowland, executive vice president of the Henry J. Kaiser Family Foundation, which studies health policy, said it had become broadly accepted “that an individual mandate is the only alternative to government provision of coverage if you hope to achieve universal coverage.”
That said, even Massachusetts officials acknowledge that their universal coverage plan is not likely to be universal anytime soon.
“There’s good evidence,” Mr. Kingsdale said, “whether it’s buying auto insurance or wearing seat belts or motorcycle helmets, that mandates don’t work 100 percent.” He added, “We’re talking about how close you can get to 100 percent, and to me it’s pretty evident you can’t get as close without the mandate as you can with it.”
----------
5 Massachusetts insurers control about 90 percent of the healthcare insurance market in the Commonwealth of Massachusetts:
#1 - Blue Cross Blue Shield
#2 - Harvard Pilgrim Health Care
#3 - Fallon Community Health Plan
#4 - Health New England
#5 - Tufts Health Plan
-
There are also national healthcare insurance companies such as United HealthCare Insurance Co., Aetna, and CIGNA.
Source: "200,000 may need to get more insurance: State healthcare law sets higher minimums" (By Alice Dembner, [The Boston]Globe Staff, January 30, 2007).
-----
Questions on Massachusetts healthcare insurance mandate program:
#1 - Will insurance be truly affordable?
#2 - Will individuals revolt when the state starts fining those without coverage next year?
#3 - Will employers maintain the insurance they now offer?
#4 - Will there be enough federal and state funding to cover rising costs?
-
The state's plan relies largely on two sources: federal funds that are committed only through June 30, 2008, and the state's free-care pool, now used to pay for charity care at hospitals and health centers.
-
Source: "MANDATORY HEALTH INSURANCE | THE FIRST YEAR: Progress and perils - Thousands more in state have coverage under ambitious program, but challenges lie ahead over funding and getting message out to all" (By Alice Dembner, (Boston) Globe Staff, April 22, 2007).
-----------
Case for health insurance mandate
The Berkshire Eagle - Editorial
Saturday, December 01, 2007
NORTH ADAMS, Massachusetts
One of the more thoughtful perspectives on health insurance mandates is published in the current issue of Health Affairs titled "Consider it Done? The Likely Efficacy Of Mandates For Health Insurance," written by Sherry Glied, Jacob Hertz, and Genessa Giogi. In presenting both the benefits and the challenges of using mandates to expand coverage, the authors make the observation that health insurance mandates are attractive to policy makers for the following reasons:
Mandates offer a way to address the problem of those who are already eligible for public programs but fail to obtain coverage, thus making coverage a more urgent concern.
Mandates level the playing field, forcing employers or individuals who have been using publicly funded services to pay their fair share of the cost of coverage.
Mandates can reduce the need for explicit public funding of new coverage, by substituting funds generated through the mandate for tax funds.
Mandates can ease insurers concerns that only less healthy people will choose to participate in a new voluntary insurance program.
Mandates can act as a legislative self-control device, binding the government to provide adequate subsidies to make compliance feasible."
They note there are already in place a number of mandates outside of heath insurance that have we have accepted for years including: automobile insurance, individual income tax (we don't typically see income tax as a mandate, but it is), child support, childhood immunization, and minimum wage laws.
The efficacy of these mandates varies: The percentage of motorists who comply with automobile insurance mandates ranges from 66 percent to 96 percent, depending on each state; the number of people who voluntarily file the correct amount of taxes they owe on time is 84.5 percent; childhood immunization compliance ranges from 85 percent for states with immunization mandates to 77 percent in states without a mandate; studies of the minimum wage laws find compliance rates of 65-75 percent, with much variation among industries. The least successful mandate appears to be child support at 30 percent, depending on income level and the quality of the relationship between the parents
The authors also suggest that the more successful mandates include several features: "Compliance is easy and relatively inexpensive; penalties for non-compliance are stiff but not excessive; and enforcement is routine, appropriately timed, and frequent."
While it is difficult to predict the efficacy of the Massachusetts health insurance mandate, there are already significant accomplishments. Since July 2006, over 200,000 previously uninsured residents now have health coverage through the expansion of MassHealth and the implementation of Commonwealth Care, the health insurance program created to make the mandate feasible. It is anticipated that thousands more will now purchase insurance through their employers. These are individuals who otherwise would have gone uninsured without the coercion of the mandate.
Recently I interviewed an uninsured woman who expressed resentment at being mandated to apply for health coverage. She explained that she's relied on non-traditional health care not covered by insurance, and she asked how could the mandate help her. After some discussion, she did acknowledge that if she developed heart disease, cancer, or if she incurred other serious illnesses, or if she suffered an accident she could be vulnerable to thousands of dollars of medical debt.
My sense is that, unable to afford health coverage, she understandably protected herself by denying how vulnerable she really felt being uninsured. At its core, effective health insurance removes the financial barriers that prevent individuals from receiving health care, and protects individuals from financial harm.
At the end of the interview, she applied for Commonwealth Care, where the premium will cost her $70 a month. When she left the office she admitted she felt secure knowing that, if needed, she could now pursue medical care without fear of medical debt.
Over the next few years we will learn a lot from our experiences with the Massachusetts health insurance mandate. But already we are seeing some early successes, and these successes should be acknowledged from both a policy and a human perspective.
Charles Joffe-Halpern is the executive director of Ecu-Heath Care and the president of the Board of Directors of Health Care for All in Boston. He can be contacted at cjoffehalpern@nbhealth.org
-----------
THE BOSTON GLOBE - Op-Ed
Single-payer healthcare is the one way
By Michael Kaplan | December 3, 2007
ALONG WITH most residents of Massachusetts, I assumed that the Massachusetts Health Reform Law was going to allow my daughter to keep her health insurance coverage after she graduated from college. The Connector Authority specified that for two years of post- dependency status, a young adult could remain on a family policy. What a relief that was. She graduated this May and is in those early stages of becoming self-supporting.
When my wife's employer, Berkshire Health Systems, informed us that my daughter's coverage would end on Dec. 31 of this year, I was shocked. It turns out that the law requires only companies that pay health insurance premiums to give the extra two years of coverage. Those companies that self-insure are governed by federal law under ERISA and are not bound by this requirement. Self-insured companies pay the health insurance companies to administer the benefit, not to insure them. So our Blue Cross Blue Shield policy seems like an insurance policy, but it is not. Berkshire Health Systems insures itself, as do national companies that employ across state lines. Many large local employers are self-insured as well. These large companies do not have to pay the extra cost to cover dependents for those two more years.
Small businesses are generally not able to take on the financial risk required to self-insure, so those companies that provide insurance to employees do have to pay the extra premiums. Whatever happened to the relief that small business was supposed to get from this reform law? Ask any small business owner and you will learn that health insurance costs for employees may have risen by as much as 50 percent since this law was passed!
My daughter has been able to get two part-time jobs, but of course she has not been offered health insurance. I am told that she may qualify for Commonwealth Care that the Connector offers under the new law.
Although the Commonwealth Care subsidized insurance is not tied to employment, coverage would be lost if she either started earning above a threshold amount or moved from Massachusetts, both likely events for a young graduate. And as a consequence of the loophole exempting many big employers from covering their employees' children for two post-college years, Commonwealth Care is likely to include more young people than expected.
This will create higher expenses for the state than originally projected, worsening the cost problem that that casts a shadow over the entire program.
Jon Kingsdale, executive director of the Connector Authority, recently said, "If we continue with double-digit inflation [in health insurance premiums] I don't think health reform is sustainable." However, there is nothing in the new law that works to control these sky-rocketing costs.
As a physician and healthcare activist for many years, I was aware that this reform law was not a panacea and did nothing to control the rapidly rising costs of private insurance that force both employers and their employees to pay more in premiums, with the insured also paying more in higher copayments and deductibles. While the reform widened the safety net for some poor families, this safety net will shred if there is not a massive infusion of new money from the state or federal governments.
Two important lessons can be learned. First, we need to sever the connection between healthcare and employment. People need continuous, portable coverage that is affordable, comprehensive, and equitable. Second, we cannot depend on the private insurance industry to provide this for us.
Piece-meal reform such as the new law will not work. Both employers and the public support the concept of single-payer healthcare. Big business is starting to realize that a single payer system will be the only affordable way to cover everyone. When will our politicians understand that their political futures will depend on supporting this kind of comprehensive reform?
Michael Kaplan is a family physician and a member of Physicians for a National Health Plan and the board of directors of the Universal Health Care Education Fund.
-----------
The NY Times - Editorial
November 25, 2007
The High Cost of Health Care
The relentless, decades-long rise in the cost of health care has left many Americans struggling to pay their medical bills. Workers complain that they cannot afford high premiums for health insurance. Patients forgo recommended care rather than pay the out-of-pocket costs. Employers are cutting back or eliminating health benefits, forcing millions more people into the ranks of the uninsured. And state and federal governments strain to meet the expanding costs of public programs like Medicaid and Medicare.
Health care costs are far higher in the United States than in any other advanced nation, whether measured in total dollars spent, as a percentage of the economy, or on a per capita basis. And health costs here have been rising significantly faster than the overall economy or personal incomes for more than 40 years, a trend that cannot continue forever.
It is the worst long-term fiscal crisis facing the nation, and it demands a solution, but finding one will not be easy or palatable.
The Causes
Varied and Deep-Rooted. Contrary to popular beliefs, this is not a problem driven mainly by the aging of the baby boom generation, or the high cost of prescription drugs, or medical malpractice litigation that spawns defensive medicine. Those issues often dominate political discourse, but they have played relatively minor roles in driving up medical spending in this country and abroad. The major causes are much more deep-seated and far harder to root out.
Almost all economists would agree that the main driver of high medical spending here is our wealth. We are richer than other countries and so willing to spend more. But authoritative analyses have found that we spend well above what mere wealth would predict.
This is mostly because we pay hospitals and doctors more than most other countries do. We rely more on costly specialists, who overuse advanced technologies, like CT scans and M.R.I. machines, and who resort to costly surgical or medical procedures a lot more than doctors in other countries do. Perverse insurance incentives entice doctors and patients to use expensive medical services more than is warranted. And our fragmented array of insurers and providers eats up a lot of money in administrative costs, marketing expenses and profits that do not afflict government-run systems abroad.
Does It Matter? If citizens of an extremely wealthy nation like the United States want to spend more on health care and less on a third car, a new computer or a vacation home, what’s wrong with that? By some measures, Americans are getting good value. Studies by reputable economists have concluded that spending on such advanced treatments as cardiac drugs, devices and surgery; neonatal care for low-birth-weight infants; and mental health drugs have more than paid for themselves by extending lives and improving their quality.
But if health care spending continues on its same trajectory, the United States will reach the point — probably several decades from now — where every penny of the annual increase in gross domestic product would have to go for health care. There would be less and less money for other things, like education, environmental protection, scientific research and national security, that may be equally or more important to the well-being of society.
Governmental budgets will face the crisis even sooner. States are already complaining that they have to crimp other vital activities, like education, to meet soaring Medicaid costs. And federal spending on Medicare and Medicaid is surging upward at rates that will cause the deficit to soar. That means politicians will have to raise taxes, severely cut a wide range of other governmental programs, or chop back the health programs themselves.
The question is: What can be done to lower both the high level of health care spending and its high rate of increase from year to year?
The Solutions
Geography. Pioneering studies by researchers at Dartmouth have shown enormous disparities in expenditures on health care from one region to another with no discernible difference in health outcomes. Doctors in high-cost areas use hospitals, costly technology and platoons of consulting physicians a lot more often than doctors in low-cost areas, yet their patients, on average, fare no better. There are hints that they may even do worse because they pick up infections in the hospital and because having a horde of doctors can mean no one is in charge.
If the entire nation could bring its costs down to match the lower-spending regions, the country could cut perhaps 20 to 30 percent off its health care bill, a tremendous saving. That would require changing the long- ingrained practices of the medical profession. Public and private insurers might need to refuse coverage for high-cost care that adds little value.
Stick to What Works. The sad truth is that less than half of all medical care in the United States is supported by good evidence that it works, according to estimates cited by the Congressional Budget Office. If doctors had better information on which treatments work best for which patients, and whether the benefits were commensurate with the costs, needless treatment could be junked, the savings could be substantial, and patient care would surely improve. It could take a decade, or several, to conduct comparative-effectiveness studies, modify relevant laws, and change doctors’ behavior.
Managed Care. For a brief period in the 1990s it looked as if health maintenance organizations competing for patients and carefully managing their care might bring down costs and improve quality at the same time. The H.M.O.’s did help restrain costs for a few years. The problem was, doctors and patients hated the system, management became much looser, and the upsurge in costs resumed. Managed care techniques are creeping back into some health plans, especially for services apt to be overused, but too heavy a hand would most likely produce another backlash.
Information Technologies. The American health care system lags well behind other sectors of the economy — and behind foreign medical systems — in adopting computers, electronic health records and information-sharing technologies that can greatly boost productivity. There is little doubt that widespread computerization could greatly reduce the paperwork burden on doctors and hospitals, head off medication errors, and reduce the costly repetition of diagnostic tests as patients move from one doctor to another. Without an infusion of capital, the transition from paper records is not apt to happen very quickly.
Prevention. Everyone seems to be hoping that preventive medicine — like weight control, exercise, better nutrition, smoking cessation, regular checkups, aggressive screening and judicious use of drugs to reduce risks — will not only improve health but also lower costs in the long run. Preventive medicine actually costs money — somebody has to spend time counseling patients and screening them for disease — and it is not clear how soon, or even whether, substantial savings will show up. Still, the effort has to be made. The Milken Institute recently estimated that the most common chronic diseases cost the economy more than $1 trillion annually, mostly from lost worker productivity, which could balloon to nearly $6 trillion by the middle of the century.
Disease Management. Virtually all policy experts want more careful coordination of the care of chronically ill patients, who account for the largest portion of the nation’s health care expenditures. Although that should improve the quality of the care they get, coordination may not cut costs as substantially as people expect. In some initial trials it has cut costs, in others not.
Drug Prices. Compared with the residents of other countries, Americans pay much more for brand-name prescription drugs, less for generic and over-the-counter drugs, and roughly the same prices for biologics. This page believes it would be beneficial to allow Medicare to negotiate with manufacturers for lower prescription drug prices and to allow cheaper drugs to be imported from abroad. The prospect for big savings is dubious.
Who Picks Up the Tab?
Pay Providers Less. With doctors dreadfully unhappy under the heavy hand of insurers, it would seem shortsighted to make them even unhappier by cutting their compensation to levels paid in other countries. But many experts believe it should be possible to tap into the vast flow of money sluicing through hospitals, nursing homes and other health care facilities to find savings.
Emphasize Primary Care. In a health system as uncoordinated as ours, many experts believe we could get better health results, possibly for less cost, if we changed reimbursement formulas and medical education programs to reward and produce more primary care doctors and fewer specialists inclined to proliferate high-cost services. It would be a long-term project.
Skin in the Game. The solution favored by many conservatives is to force consumers to shell out more money when they seek medical care so that they will think harder about whether it is really necessary. The “consumer-directed health care” movement calls for providing people with enough information about doctors and treatments so that they can make wise decisions.
There would most likely be some savings. A classic experiment by Rand researchers from 1974 to 1982 found that people who had to pay almost all of their own medical bills spent 30 percent less on health care than those whose insurance covered all their costs, with little or no difference in health outcomes. The one exception was low-income people in poor health, who went without care they needed. Any cost-sharing scheme would have to protect those unable to bear the burden.
And consumer-driven plans have limitations. Most health care spending is racked up by a small percentage of individuals whose bills are so high they are no longer subject to cost sharing; they will hardly be deterred from expensive care they desperately need. Moreover, few consumers have the competence or knowledge to second-guess a doctor’s recommendations.
Single Payer. Deep in their hearts, many liberals yearn for a single-payer system, sometimes called Medicare-for-all, that would have the federal government pay for all care and dictate prices. Such a system would let the government offset the price-setting strength of the medical and pharmaceutical industries, eliminate much of the waste due to a multiplicity of private insurance plans, and greatly cut administrative costs.
But a single-payer system is no panacea for the cost problem — witness Medicare’s own cost troubles — and the approach has limited political support. Private insurers could presumably eliminate some of the waste through uniform billing and payment procedures.
•
By now it should be clear that there is no silver bullet to restrain soaring health care costs. A wide range of contributing factors needs to be tackled simultaneously, with no guarantee they will have a substantial impact any time soon. In many cases we do not have enough solid information to know how to cut costs without impairing quality. So we need to get cracking on a range of solutions. The cascade of knowledge flowing from the human genome project, new nanotechnologies and the advent of treatments tailor-made for individual patients may well accelerate, not mitigate, the rise in medical spending. If we want the benefits, we will need to make them affordable.
----------
The Boston Globe: Op-Ed
JAMES ROOSEVELT JR. AND CHARLES D. BAKER
How to control healthcare costs
By James Roosevelt Jr. and Charles D. Baker
December 1, 2007
THE HEALTHCARE reform law has done a great job of expanding access to healthcare, and Massachusetts is well on its way to meeting the goal of ensuring healthcare coverage for every resident. Over 200,000 individuals who were uninsured at the beginning of this year have health insurance today.
A major challenge to ensuring that every resident continues to have access to coverage is the rising cost of healthcare. Rising costs threaten the state's ability to continue providing coverage to low-income individuals and squeeze businesses. For those of modest incomes, the requirement that they must purchase health insurance makes rising healthcare costs particularly burdensome.
Experts estimate that healthcare spending in Massachusetts rose from $46.5 billion annually in 2002 to $62.1 billion annually in 2006. That's a 33 percent increase in just four years. Understanding what's driving healthcare costs is the first step toward controlling them.
Senate President Therese Murray has proposed an interesting idea to provide more information on what is driving healthcare costs, calling for a public hearing on any premium increases above 7 percent in any given year.
The Senate president is right; we need to have a broad discussion on what's driving healthcare costs. On Monday, we and several other health plan leaders will be announcing the following:
Public hearings on cost drivers. To shine a spotlight on underlying healthcare costs and to provide a full representation of the entire market, we recommend that the state's health plans be required to participate in an annual public hearing on healthcare costs - no matter what their rate increases are - to outline the factors contributing to any changes in premiums, including their projected medical expenses due to provider reimbursement rates, patient utilization, administrative costs, capital investments, and efforts to reduce the rate of growth. Health insurance premiums are driven by healthcare costs, so it is important that hospitals, health centers, physician practices, and pharmacies participate in these hearings to explain the factors contributing to their rising costs, including greater utilization of technology, increases in consumer demand, and higher reimbursement rates.
Public reporting of healthcare revenues and expenses. Consumers and employers have every right to know where their premium dollars go. While this information is reported to the state, it is not easy to find. Beginning this week, our health plans and several others will voluntarily disclose in a consumer-friendly format their financial data, including total revenues, administrative costs, and surpluses and reserve levels, along with what they pay for medical costs for their insured members. Hospitals should also make publicly available data disclosing total inpatient and outpatient service revenue, total patient expenses, total capital expenses, total administrative expenses, surplus revenue, and endowment levels at a similar level of detail to that being released by health plans. While much of this data is currently filed with various state entities, it is important that hospital leaders come together to disclose this information in a format that is more easily understandable and more accessible to the public than it is today.
A public forum to find solutions. Making better use of existing healthcare resources and keeping healthcare affordable will require the participation of everyone in healthcare, not just one or two groups working alone. We don't pretend to have all the answers and believe it is important that our partners in the healthcare community - hospitals, physician groups, community health centers, consumer organizations, employers, and state policy makers - work with us to convene a series of forums to identify and outline additional measures that control healthcare costs while maintaining or improving quality of care.
Murray has started a debate that should lead to an analysis about healthcare costs and should start by everyone having to answer the question, "Why are your costs going up and what are you going to do about it?" The future of the state's healthcare reform - and the people depending on it - is at stake.
James Roosevelt Jr. is president and CEO of Tufts Health Plan and chairman of the Massachusetts Association of Health Plans. Charles D. Baker is president and CEO of Harvard Pilgrim Health Care and is past-chairman of the Massachusetts Association of Health Plan.
----------
NEWS ARTICLE: THE BOSTON GLOBE -
6-figure pay for care plan overseers
Salaries at new state agency stir concern
By Andrea Estes, Globe Staff | January 27, 2007
Employees of the new state agency established to provide health insurance to the state's low-income residents have been hired at an average salary of $111,000 a year, with 12 of the 22 staff members making more than $100,000 and six earning more than Governor Deval Patrick and his Cabinet secretaries.
The state's landmark universal healthcare law, approved last year to provide affordable coverage to the state's approximately 500,000 uninsured residents, has created a bureaucracy with a salary scale like that of the Massachusetts Turnpike Authority or the Massachusetts Port Authority, two quasi-independent agencies that Patrick and former governor Mitt Romney have railed against for their overly generous compensation packages.
With the agency struggling to provide the affordable premiums the legislation promised, some community leaders and lawmakers involved in the program's development said they were surprised by the salaries, which are being paid initially through a $25 million appropriation by the Legislature. Eventually the Commonwealth Health Insurance Connector's administrative costs will be funded by insurance companies through a surcharge on premiums.
"I am going to call in the director and find out where they're spending the money," said House Speaker Salvatore F . DiMasi, one of the architects of the legislation. "We don't want administrative costs to be too high. We want the money spent efficiently."
Senator Richard Moore, who helped shepherd the bill through the Legislature, said : "If they're paying large salaries, the $25 million isn't going to last long."
A spokesman for the Connector said the salaries reflect "each individual's ability, experience, and responsibilities.
"People who have come to work at the Connector did so to be involved in something exciting, challenging, and historic, and for some that means earning less," said Richard Powers, the Connector's director of public affairs, who pointed out that five of the eight senior staff members are making less than they did at their previous jobs.
He said most of the employees had an extensive background in the health insurance industry.
Under the health insurance law, approved last April, all adults must obtain insurance coverage by July 1 or pay a penalty, unless they secure a waiver by proving they can't afford insurance.
The law established the Connector, which has a staff of 22 employees and is overseen by an unpaid 10-member board.
Last week, the board postponed a vote to set minimal coverage requirements, after learning that it could cost the average individual $380 a month.
The Connector's executive director, Jon Kingsdale, who earns $225,000 a year, determined the compensation for other employees.
The second-highest paid, deputy director Rosemarie Day, was hired at $195,000 a year, but her salary was reduced to $175,500 when she opted for a four-day week.
Some members of the 10-member board that oversees the Connector were also surprised when Kingsdale informed them of the high salaries and administrative costs, including a recently awarded $4 million advertising contract to educate the public, according to one board member.
"We had to go with the people he chose," said the board member, who spoke on condition of anonymity because members are not authorized to speak to the media. "We didn't have time for people to learn on the job. We needed people who at least understood the industries they were dealing with. The real problem is the industry pays their folks really high, and to get them to come over -- they're not going to do it for a huge wage cut."
Ultimately, under the state's plan, insurers will fund the salaries and other administrative expenses by paying a surcharge of 4 to 5 percent on the premiums they collect as a result of the program. Some have raised concerns that insurers will pass along the cost to consumers in higher premiums.
"The cost of the salaries will be part of the cost of the insurance, " asserted David Tuerck, executive director of the Beacon Hill Institute, a conservative think tank.
"The Connector was created to take the cost off budget and put it onto the insurance companies," he said. "I would describe [the surcharge] as a disingenuous attempt to mask the cost of healthcare reform."
A spokesman for the Massachusetts Association of Health Plans was not available to comment on the surcharge.
Several lawmakers said that they did not intend to create a cumbersome new bureaucracy when they passed the landmark law.
According to DiMasi, the House specifically pressed to make the Connector a state agency, part of the Secretariat of Administration and Finance, so it would be directly accountable to the governor.
Others, particularly members of the Senate, argued that the Connector should be independent so it could have more flexibility in hiring and compensation.
The 10-member board is composed of four state officials, three appointed by the governor and three by the attorney general.
Eric Fehrnstrom, a spokesman for Romney, said the former governor pushed for an independent authority because it was the most efficient way for uninsured employees to buy health insurance on a pretax basis.
"The quasi-governmental entity structure was selected due to the singular mission of the Connector, which is to maximize the number of people with insurance," Fehrnstrom said. "No other state agency is tasked with this assignment."
John McDonough, executive director of Health Care for All and a former state representative, said he does not believe the compensation is too high.
"Compared to what people make in state government, these salaries are high, but not compared to what comparable people make in a commercial insurance world," he said. "If they didn't pay these salaries, I don't believe they would be getting the quality people they need to do this highly complex operation."
But McDonough cautioned that the financial underpinnings of the system are so precarious that the Connector may not be able to sustain itself as envisioned.
"The whole structure is fraught with uncertainty," he said. "This is a challenging task requiring a lot of thoughtful delicate balancing to make the coverage favorable enough so people want it and affordable enough so people can buy it.
"If they fail to do that and people don't buy the policies, they won't have the revenue to support the operation."
A spokesman for Patrick, whose salary is $140,535 a year, declined comment on Connector salaries.
----------
CAMPAIGN NOTEBOOK
Obama says his health package does more
By Sally Cragin, Globe Correspondent | November 25, 2007
COUNCIL BLUFFS, Iowa - Democratic Senator Barack Obama of Illinois, seeking to distance himself from his leading rivals, touted his healthcare expansion package as doing more to cut costs and deal with root problems facing consumers "than any other proposal in this race."
Obama's two main rivals for the Democratic presidential nomination - Senator Hillary Clinton of New York and former senator John Edwards of North Carolina - have offered universal healthcare plans, while his stops short of mandating everyone have health insurance.
Obama routinely describes his rivals' plans as similar in thrust, but he began sharpening those differences as he opened his latest campaign swing yesterday.
"Cost is the number one reason that 47 million Americans do not have health insurance and thousands more are edging toward bankruptcy every day," Obama told a town hall-style meeting of about 350 people at a Council Bluffs high school. "That is wrong, and it's why my plan does more to cut the cost of health insurance than any other proposal in this race."
Obama sought to distance requirements in his rivals' plans that consumers must buy health insurance, saying that thinking is misplaced.
"What I have said repeatedly is that the reason people don't have health insurance is not because they don't want it, it's because they can't afford it," said Obama.
While Obama conceded plans for the leading rivals are similar, he said the insurance mandate is a key difference.
While Clinton has built a substantial lead in national surveys of the Democratic field, the race in Iowa among Obama, Clinton, and Edwards is extremely tight heading into the state's leadoff precinct caucuses, the traditional opening test of the presidential nominating season.
----------
'Sicko' chronicles sick health system
Letters
Saturday, December 01, 2007
I implore all Berkshire Eagle readers who have not seen the movie "Sicko" to rent it, especially if not convinced that the American health care system is shameful compared to those in the other advanced countries of the world. We deserve a system at least as good.
I also wish to thank Dr. Susanne King for her many Eagle columns advocating a single-payor system. Surely, its time has come.
ALLAN SEPPA
Pittsfield, Massachusetts
----------
News Article:
Clinton, Obama: Coverage vs. cost
By MIKE GLOVER
The Associated Press
Monday, Nov. 26, 2007
DES MOINES, Iowa – Hillary Rodham Clinton and Barack Obama intensified the bickering yesterday over their competing health plans, reflecting the crucial stakes as Iowa's leadoff caucuses in early January approach.
Clinton said Obama's proposal was "crafted for politics" and the latest example of his shifting policy positions. Obama said much the same of her approach.
"Senator Obama and I have been having a debate about health care for a couple of days and it's a very important debate," Clinton said in a telephone interview with The Associated Press. "The difference is my health care plan covers every American and Senator Obama's plan will not."
Obama focused on Clinton's proposal to require that people buy coverage. His approach carries no such mandate, which he says is potentially costly for consumers.
"The reason Americans don't have health insurance isn't because they don't want it, it's because they can't afford it, which is why my plan doesn't have a mandate and goes further in cutting costs than any other proposal offered in this race," Obama said during a campaign stop to discuss health care issues. He said people could save up to $2,500 a year under his plan €" more than under any of his rivals' plans.
Clinton disputed that, saying very similar cost savings are built into her plan.
"He leaves 15 million people uncovered," the New York senator said. "It's a plan crafted for politics, not for people."
Obama responded: "Hillary's idea is that we should force everyone to buy insurance. But this is yet another issue where she is not being straight with the American people because she refuses to tell us how much she would fine people if they couldn't afford insurance."
The Illinois senator said it is another instance of political maneuvering on Clinton's part. "So unless she can answer those questions, this is yet another calculation that's more about getting through an election than actually solving the health care problems," he said.
Obama credited the new criticism from Clinton to his improved poll numbers in Iowa.
"This is politics," Obama said in an interview with The Associated Press. "This is her apparently being concerned about her standing in Iowa."
Obama's aides have suggested the candidate would leave it up to the states to consider imposing a mandate; some have begun to move in that direction.
"That is unworkable. Can you imagine 50 state bureaucracies, the billions of dollars wasted on redundancy?" Clinton said. "This is an American problem and we need an American solution."
In recent appearances, Obama has revived criticism of Clinton's failed effort to overhaul the health care system in the 1990s when she was first lady. He also has accused her of being too secretive.
"An important part of this effort will be creating an open, transparent process so the American people feel informed about and invested in what we're trying to do," Obama said. "When the American people are paying attention and are brought into the process, there's nothing we can't achieve."
Clinton said Obama tried to convince voters at first that his plan would offer universal coverage, then acknowledged it would not cover everyone and now is trying to justify an approach that falls short of universal coverage.
The Obama campaign circulated a memo to reporters yesterday demanding to know how Clinton would enforce the mandate, noting that one state €" Massachusetts €" has taken that route and consumers that do not get coverage lose their personal tax exemption, a $219 cost.
"Now he's trying to justify the fact that he doesn't cover everyone," Clinton said. She said Obama's plan would leave 15 million people relying on expensive emergency room coverage.
The sharp tenor of Clinton's remarks, and her direct engagement of Obama, reflect the tight race in Iowa. Clinton has amassed a big lead in national polls and a win in Iowa could give her an enormous amount of momentum. That leaves her rivals viewing Iowa as the best or only place to derail Clinton's campaign.
----------
Insurers doom reform effort
The Berkshire Eagle - Letters
December 04, 2007
I read Dr. Susanne King's account of Blue Cross Blue Shield executive William C. Van Fassen's $16.4 million retirement package and $3 million salary with a combination of astonishment, outrage, anger, and disgust. ("Our health care dollars at work," op-ed, Nov. 28).
Individuals, businesses, and town governments throughout the state paid our hard-earned dollars to fund Mr. Van Fassen's package. But on reflection, we also owe Mr. Van Fassen our thanks for showing us so dramatically how insurance companies create an unnecessary layer of administrative costs as they skim money away from patient care.
Mr. Van Fassen's outrageous income also demonstrates how our current health care reform strategy is destined to fail. Already over $100 million short of funds, insurance company executives can still divert money away from patient care and into their own pockets. As long as we have a system that includes insurance companies, money will continued to be channeled into executive salaries and other administrative expenses that do nothing to improve anyone's health.
I agree with Dr. King and the majority of doctors in Massachusetts that we need to eliminate the multiple insurance companies and have a "single-payer" to take in our health care funds and distribute them to the providers of health care. I plan to contact my legislators about my support for single-payer, and I hope others in our community do so as well.
RICHARD M. BERLIN, M.D.
Lenox, Massachusetts
----------
News Article:
New strategy for health care cost cuts
By Hillary Chabot, Eagle Boston Bureau
Tuesday, December 04, 2007
BOSTON — The top health insurance providers in the state yesterday suggested opening the books to cut spiking costs in health insurance.
The proposal was one that could save the state several billion dollars in health care costs, according to Massachusetts Association of Health Plans President Marylou Buyse.
"We're going to look into cost savings and what we can do to help keep premiums affordable," Buyse said.
The suggestions were sparked by Senate President Therese Murray, D-Plymouth, who will file legislation next year in an effort to cut health care costs.
The state's new universal health care law already has spawned a $147 million gap in the budget as nearly 200,000 people signed on to Commonwealth Care, the state subsidized health care plan. Health care costs have increased by 33 percent statewide in the past four years, from $46.5 billion in 2002 to $62.1 billion in 2006.
"The long-term success of the bill depends upon us adopting measures for cost control," said Jim Roosevelt, president of the Tufts Health Plan.
Senate Ways and Means Chairman Steven C. Panagiotakos, D-Lowell, said premium increases should be put through a public hearing process, and the public should be able to see where their money is going.
"The more transparency there is in the system, the better off we are," Panagiotakos said.
The group also suggested publishing the salaries and compensation packages of their top officials in health insurance, as long as the hospitals also published the salaries of their top officials.
The move comes as news of Blue Cross Blue Shield CEO and Chairman William Van Faasen pocketed $16.4 million in retirement benefits when he stepped down last month.
"A lot of people have been frustrated in recent weeks when they see the head of Blue Cross Blue Shield get a huge payout and they are struggling with their own health care costs," said state Sen. Benjamin B. Downing, D-Pittsfield.
The insurers' suggestions included: a prohibition on billing insurers for avoidable mistakes, public reporting of preventable medical errors, a repeal of no-longer-effective mandated benefits, and comparative studies of medical services.
The Health Care Quality and Cost Council also should hold hearings, originally at Murray's suggestion, if premiums rise more than 7 percent.
State Rep. Jamie Eldridge, D-Acton, said that, although the suggestions are good, health insurers also need to look at their own issue.
"If you have a doctor who is only paid to see patients for 10 minutes, the likelihood of errors increase," Eldridge said. "They need to restructure the process so doctors who keep patients healthy are rewarded."
Lawmakers said they would study the suggestions and incorporate them when they can.
"We're certainly going to look at any good ideas about cost containment and quality improvement," said state Sen. Richard Moore, D-Worcester, who is chairman of the committee on health care financing.
----------
"Health savings accounts for poor tested"
By KEVIN FREKING, Associated Press Writer
Saturday, December 15, 2007
The popularity of health savings accounts for the poor will be put to the test in Indiana under a program approved Friday by the Bush administration. Under the plan, someone making $20,000 a year could get health coverage for about $19 a week.
Bush has long pushed health savings accounts as a way to slow the rising cost of medical care and extend basic coverage to the uninsured.
Under the Indiana program, eligible residents can pay up to 5 percent of their incomes into state-subsidized "Personal Wellness and Responsibility Accounts" that cover their initial medical expenses up to $1,100. Once that deductible is reached, private insurance purchased by the state kicks in.
Eligibility is limited to adults with incomes below twice the federal poverty level. The poverty level is now $10,210 for an individual and $20,650 for a family of four.
The waiver is the first of its kind for the Medicaid program, a state-federal partnership that provides health coverage to the poor and disabled.
Indiana officials said they've already received inquiries from more than 1,000 people interested in applying.
The program will be monitored closely because of the philosophical divide among lawmakers about the value of health savings accounts for the poor. Many say such accounts work best for healthier and higher-income people with low medical expenses.
Judith Solomon, senior fellow at the Center on Budget and Policy Priorities, said she doubts that many people making $10,000 a year can afford to pay $500 for health insurance. She said that about 50,000 people lost Medicaid coverage in Oregon after that state got permission to raise insurance premiums to $20 a month.
"You can say it's better than nothing, but I just don't see how many of those folks will be able to afford it," Solomon said.
Indiana has allocated up to $114 million for the program in 2008 after its legislature voted to raise state taxes on cigarettes from 55.5 cents to 99.5 cents a pack.
The state is encouraging employers to contribute to their workers' accounts. Any money left at the end of the year can be rolled over to offset the following year's contributions if the beneficiary obtains certain screenings and services that help prevent illness.
"This is a big step forward that will lead to approximately 120,000 uninsured Hoosiers having the peace of mind of health insurance," said Indiana Gov. Mitch Daniels, a Republican who once served as Bush's director of the Office of Management and Budget.
-
On the Net:
Healthy Indiana Plan: http://www.hip.in.gov
----------
THE BOSTON GLOBE: Op-Ed: SUSAN F. WOOD
A public health system defeated at the hands of ideology
By Susan F. Wood, December 17, 2007
THE STATE Children's Health Insurance Program, which provides working families with low-cost health insurance coverage, is now in limbo - on short term extensions by Congress and just vetoed again by the president. This confronts states with difficult choices on how to continue providing health coverage for kids when the funding from Washington just isn't enough.
This latest affront to public health also comes at the same time that the price of birth control pills on colleges campuses has skyrocketed from $5-10 a month to $40 a month or more as an unintended consequence of a recent change in federal law. There is an easy and free technical fix that Congress or the Department of Health and Human Services could make, but this administration does not support allowing companies to sell birth control pills at a discount to colleges, universities, and other safety net programs.
These are just two of the more visible defeats that healthcare has suffered during this administration. At a deeper level, the low priority healthcare gets from President Bush is reflected in his failure to staff important health-related positions with qualified individuals willing to provide science-based advice.
Currently, the Department of Health and Human Services, the lead department that includes all of our national health agencies, lacks a permanent assistant secretary for health, assistant secretary for children and families and a surgeon general. All of these key senior positions are held by temporary appointees, some highly qualified, others not, but none with the ability to truly move us forward by providing sound advice and having the ear of decision-makers.
The Food and Drug Administration lacked a permanent commissioner for over half of the current administration, and currently the Centers for Medicare and Medicaid - which runs the State Children's Health Insurance Program - also has no permanent leader.
Over two years ago, I resigned my post as assistant commissioner of women's health at the FDA because of the agency leadership's disregard for scientific decision-making regarding emergency contraception.
Unfortunately, since then, I have only seen mounting evidence of this administration putting politics before science. Key leadership positions in our health agencies are left vacant for unacceptable time periods or filled with individuals who advance an ideological agenda and show a disregard for scientific integrity. This pattern is troubling because it threatens the objectivity that guarantees the health and safety of American families.
Just a year after my resignation, Dr. Richard H. Carmona resigned as surgeon general. He later revealed that the administration asked him to censor his reporting on embryonic stem cell research, contraception, and the unrealistic proposition of abstinence-only sex education. This position has been vacant for over a year and in October Dr. Steven K. Galson - who was one of those at FDA who initially blocked the provision of emergency contraception over-the-counter - was given the temporary appointment of acting surgeon general.
More recently, President Bush appointed Dr. Susan Orr, an opponent of family planning, as acting deputy assistant secretary for population affairs where she is charged with advising on issues regarding population affairs and overseeing the only federal grant program dedicated solely to providing individuals with comprehensive family planning and preventive health services.
By appointing a leader who clearly does not support contraception, the administration is once again neglecting the health needs of millions of Americans, particularly those who are low income and rely on public programs to get access to preventive healthcare, including contraception and pap tests.
To ensure the health of our families we need strong, consistent leaders who value the integrity of science, make decisions on the best available information, and support prevention. Without that leadership, we will not succeed in promoting the health of all Americans. We shouldn't have to wait for a change in presidential leadership.
Susan F. Wood is research professor at the George Washington University School of Public Health and Health Services. She served as assistant commissioner for women's health at the Food and Drug Administration from 2000 to 2005 and is advising Hillary Clinton on health issues.
----------
-

Dan Reitzas's firm will pay a fine for dropping insurance.
-
"Firms find ways around state health law"
By Alice Dembner, (Boston) Globe Staff, December 23, 2007
To comply with the new state insurance law, a Burger King franchisee in Boston expanded coverage from just his salaried staff to all full-timers. To control his costs, he halved the share he pays. Only three of the 27 newly eligible employees took the insurance; others say they can't afford it.
A large human service provider toughened eligibility for coverage in response to the new law, requiring employees to work 30 hours a week to qualify. That took away the option of work-based coverage for nearly 100 low-wage workers, but made them eligible for cheaper, state-subsidized insurance. It could reduce the company's costs while increasing the state's.
Another employer split his firm into separate corporations, each with fewer than 11 full-time employees, according to his insurance broker. That way he does not have to offer insurance, nor pay a fine.
Businesses from Boston to the Berkshires are responding to the state's landmark health insurance initiative in ways that could help it succeed - or stumble.
Policy makers are watching and waiting, but said they will act if many employers dodge their obligations.
In the first nine months of this year, according to the latest state figures, about 45,000 workers and their families gained insurance because employers picked up part of the tab. That number represents a small but significant chunk of the 293,000 newly insured state residents, a total that puts Massachusetts between half and three-quarters of the way toward its goal of covering nearly every resident.
Yet some employers are taking actions that could shift costs to the state or leave more people uninsured, potentially upsetting the delicate balance of responsibility on which the initiative rests, according to interviews with more than 20 companies, insurance brokers, and trade organizations.
When drafting the universal insurance law, "we purposely did not raise employer taxes" to pay for insurance, said Senator Richard T. Moore, cochairman of the Legislature's Committee on Health Care Financing, who plans oversight hearings within a few months.
"We thought we were treating employers fairly, and I commend the overwhelming number of employers who are doing the right thing," he said. "If some are not going to respond fairly, we'll find ways to structure the law so the loopholes get closed."
Businesses with 11 or more full-time equivalent workers are now required to offer insurance or pay a fine. The law also bars employers from offering higher-wage workers better health benefits than low-wage employees. In addition, workers with access to employer-subsidized insurance are now barred from getting state-supported coverage, and will be excluded from the state's free care program starting in April.
The provisions were designed to ensure that as many workers as possible get coverage through their employers in a state where about 70 percent of the 200,000 businesses offer insurance benefits.
For years, Doug Barlow and his business partner had paid 100 percent of the insurance cost for 11 full-time salaried workers at their three Burger King restaurants in Boston. The new law's antidiscrimination provisions led them to offer insurance to 27 hourly employees. But the potential cost - nearly $1,100 per month for family coverage - pushed them to cut the firm's contribution to 50 percent.
"I was prepared for a lot more people coming into our plan, but it didn't happen," said Barlow. Other employers said they are seeing the same pattern - expanded eligibility that does not lead to many more insured individuals.
"For most working-class people, regardless of whether the company pays part of the premium, it's very expensive," Barlow said. "Some full-time people said they'd done the math and it is cheaper for them to pay the state penalty than pay their half of health insurance."
The law requires individuals to obtain insurance by Dec. 31, if the state deems it affordable, or pay a penalty of $219. Next year, the penalty will rise.
Rebecca Posada works the counter at the busy Burger King in Center Plaza. Although she's been uninsured for the five years she's worked there and would like coverage, she is refusing Barlow's offer.
"I don't make enough" to pay $46 a week in premiums, said Posada, 26, during a morning break. She hopes to continue getting free care at the East Boston Neighborhood Health Center, and may be able to avoid the state penalty because of her low income.
Vinfen, a 2,000-person company that runs programs for mentally ill clients statewide, took a different approach that its officers said is designed to help low-wage workers. New employees now have to work 30 hours a week to qualify for insurance, up from 20.
"It's not a knee-jerk effort to reduce our costs," said Tim De Araujo, vice president of human resources. "By denying them eligibility to our plan, we gave them eligibility to the state plan. We felt this was the right thing to do."
De Araujo said he would like to see the state offer employees a choice of their employer plan or the state plan, whichever is more affordable. Two-thirds of their employees earn less than $24,000 a year, which would qualify them for state-subsidized coverage.
Separately, Vinfen renewed an offer of coverage, with a 70-75 percent subsidy, to 650 existing employees who were eligible but not enrolled. Only 72 signed up.
Some other firms have similarly tightened eligibility to control costs or try to shift employees to state plans, said Christopher DeLorey, a director of Telamon Insurance & Financial Network, and several other brokers.
Policy makers and analysts are concerned that this pattern could boost enrollment in the state-subsidized plan, which is already far above predicted levels. The bulk of the newly insured so far are covered by state-funded programs.
"Both the individual and the employer benefit" from the shift, said Michael Widmer, head of the Massachusetts Taxpayers Foundation, a business-funded financial watchdog. "But we don't have the public dollars to fund this."
Some additional public money is coming from companies required to pay fines of $295 per employee under the law because they don't offer insurance.
Northeast Knitting Mills, a small sweater factory in Fall River, dropped coverage in February because the fourth-generation family owners could no longer afford it, said president Dan Reitzas. He will pay a $13,000 fine, which is about 6 percent of his expenses, he said, but far less than the $50,000 he was paying for insurance. He is helping employees get a tax break on privately purchased insurance.
But other firms are avoiding fines by designating their employees as independent contractors or using other questionable means, employees and brokers said.
Paul Pietro, chairman of the Mid-State Insurance Agency, said he helped one of his clients set up separate corporations for each of its Massachusetts locations. Each then had fewer than 11 employees, so the insurance law did not apply. "It's a loophole," said Pietro, who declined to identify the client. Pietro said his other clients are paying the fine or expanding insurance offerings.
Moore said he had heard of similar cases. "If it's a few employers, we could publish a list of the folks using different schemes to avoid their responsibility and let their customers know," he said.
Healthcare advocate John McDonough has another suggestion: Charge those companies a large fee if many of their employees get state-subsidized insurance.
----------
-

(Jay Premack for The Boston Globe)
-
Kerry Weems, acting administrator, Centers for Medicare and Medicaid Services.
-
Medicare chief on road again to plug prescription drug plans
-
December 23, 2007
January will mark the start of the third year of Medicare Part D, the government prescription drug benefit. But after two years, many consumers still find the drug benefit confusing. Consumers Union, the nonprofit that publishes Consumer Reports, recently said a government-administered benefit would save millions compared with the current system in which drug and insurance companies run private plans. Globe reporter Jeffrey Krasner recently spoke with Kerry Weems, acting administrator of the Centers for Medicare and Medicaid Services, when his Medicare bus stopped at a senior center in Charlestown, about how to choose the best drug plan before the 2008 open enrollment ends Dec. 31.
Q: If you've had a Part D drug plan for the last two years, how should you approach your choice this time around?
A: Beneficiaries will get a notice of changes directly from their drug plans. They should look at that. We're encouraging everybody to shop around even if they're happy with their plans. The way to shop around is to go to our website, medicare.gov. They should have a list of their medications. Go to the website, put in those drugs. The plans in your area will come up. The next question to ask is, are the plans convenient? Is there a drug store close to me? Do I want to get my drugs through the mail? Then they should look at cost. The website will show them their monthly expenses.
Q: Are most people seeing prices go up or down? Avalere Health recently published a study saying those who stay with the same plan are seeing prices go up around 20 percent.
A: Prices are very stable. The average premium is $25. The Avalere study looked at a couple of particularly low-cost plans, and those plans have low-income beneficiaries moving in and out of them. That's not as clean a study as we'd like to see. Also, with very low-cost plans, a couple dollars change can produce 20 percent increases. In dollar terms, it's not that large.
Q: In 2006, the first year of Part D, we had more than 40 plans in Massachusetts. For 2008, we're up to 51. What do you think about that level of choice? At some point does choice become a burden?
A: We want to make sure a consumer can sort these things out. If they use our webfinder tool, the top three plans will come out.
Q: Will we reach a time when a bus tour and an outreach program won't be necessary to get people to sign up for Part D?
A: One of our primary reasons for the bus tour this year is to sign up low-income beneficiaries who qualify for extra help. We're targeting ZIP codes where our low-income beneficiaries need to sign up.
Q: What can people do if they're going to fall into the "doughnut hole," the coverage gap where you have to pay out-of-pocket for drugs?
A: Many plans cover generics through the coverage gap. For a lot of people, that feature gives them the help they need.
Q: Consumers Union recently came out in favor of a government-administered Part D drug plan, saying it would save even more money. What's your opinion?
A: I disagree. To save money, you have to have a formulary of drugs covered under the plan. You have to choose which drugs you want to cover. The government would have to set up that formulary. We'd have to hire a company to do it, or hire a big bureaucracy to do it.
Q: You've already got one.
A: Actually, I don't have a big bureaucracy. There are only 4,600 people in the Centers for Medicare and Medicaid Services that administer $600 billion. That's a pretty small bureaucracy. Then the next big thing that would happen is a congressman would write in and say,'Why isn't this drug on the formulary?' " Part D has depoliticized individual drugs. I don't get mail about how come you cover this drug or that drug.
Q: What else do readers need to know if they haven't yet chosen a drug plan for 2008?
A: They should take time. I'd encourage your readers to make this a family event. Have a conversation with family members about your drug plan.
----------
-

-
"N.H. Democrats, GOP sharply divided on healthcare: Differences stark on government's role, poll finds"
By Brian C. Mooney, (Boston) Globe Staff, December 26, 2007
Most Americans believe healthcare is a critical issue the next president must tackle, but in New Hampshire, the first primary state, there's a sharp partisan split over government's role in making healthcare available. As a likely battleground, the Granite State could be a bellwether on the issue in next November's election.
The stark difference between the parties is reflected in the findings of a Boston Globe poll of likely voters in the Jan. 8 New Hampshire presidential primary - 80 percent of Democrats polled say providing health coverage is government's responsibility; only 30 percent of Republicans agree. Moreover, it explains the dramatically divergent healthcare proposals of the candidates - Democrats would move toward universal coverage and a larger government role; Republicans generally favor tax incentives to expand private insurance and restrain costs through market forces.
The nation's $2.2 trillion annual healthcare system is a balky hybrid, combining government insurance, reimbursements, and tax incentive programs with private insurance mostly offered through employers.
Healthcare accounts for nearly one-sixth of the nation's gross domestic product, and the government pays, directly or indirectly, for about half of the cost. Moreover, costs have increased at nearly twice the rate of everything else in the US economy since World War II, and an estimated 46.5 million Americans under the age of 65 have no health insurance today.
"It's a carefully constructed bomb with all these wires," said Thomas P. Miller, a resident scholar at the conservative American Enterprise Institute and a member of the National Advisory Council for Healthcare Research and Quality. The challenge in reforming healthcare, Miller said, is determining "which wire to cut first without blowing the whole thing up."
Broad consensus is difficult to reach in Washington because insurers, physicians, hospitals, consumer groups, and pharmaceutical companies have contradictory interests and strong lobbies. "All the interests intersect, and they will complain about their ox being gored," Miller said.
Public health policy researcher Kenneth E. Thorpe said Democratic candidates in general would move toward universal coverage and focus on improving the affordability of healthcare. They would also emphasize prevention and treatment of chronic diseases, such as diabetes, cancer, heart disease, and asthma.
Nearly 80 percent of healthcare spending is on patients with one or more chronic ailments, said Thorpe, an Emory University professor and former Clinton administration health official. Obesity, he said, is responsible for about a third of the growth in health costs in the United States in recent years, Thorpe said.
Republicans, meanwhile, "would provide marginal incentives for people to buy insurance," along the lines of President Bush's proposals to expand health coverage, he said.
Republicans also tend to favor issuing Medicaid money to states in block grants to encourage innovative state programs to expand coverage. A core GOP tenet also includes providing transparency for consumers by requiring more public information about treatment success rates and the cost of services negotiated between insurers and providers.
Democrats would raise taxes on the wealthiest Americans to offset the cost of their healthcare plans - John Edwards's cost estimate is up to $120 billion; Hillary Clinton's projected $110 billion; and Barack Obama's up to $65 billion. Bill Richardson contends that savings from expanded preventive programs would offset the $110 billion increase from his program.
The Democratic plans would expand the government's role substantially. Edwards, a former North Carolina senator, and Clinton, senator of New York, would require insurance for all Americans and would expand the federal employee health plan by making a version of it available to more citizens.
Obama, an Illinois senator, would utilize the federal health plan and mandate coverage for all children, but not for all adults. Edwards would provide tax credits to families and establish regional "healthcare markets," or health insurance pools, for businesses and individuals to purchase less expensive policies.
The Clinton approach would also offer the choice of a public plan similar to Medicare and provide tax credits to business. Richardson, the governor of New Mexico, would lower the Medicare eligibility age to 55, expand coverage of children and the poor, and offer tax breaks for companies and individuals obtaining their own insurance.
Senator Joseph Biden of Delaware would extend coverage to all children, allow sliding-scale "buy-in" options, based on income, to the federal employee program or Medicare for persons 55 to 64 and provide a federal reinsurance program to cover catastrophic illness. Senator Chris Dodd of Connecticut would create a "Universal HealthMart," based on the federal employee plan, in which companies and individuals would buy insurance on an income-based sliding scale. Representative Dennis Kucinich advocates full national health insurance similar to the Canadian and Medicare models.
Among Republicans, the plans also vary, but they emphasize private-sector solutions.
Mitt Romney, for example, incorporates elements of the reform plan he helped push through while governor of Massachusetts, seeking to create incentives for improvements at the state level, using Medicaid block grants and federal funds now earmarked to reimburse states for care of the uninsured. Most of those funds would be used to cover the uninsured in new subsidized private insurance plans, according to Sally Canfield, policy director of the Romney campaign.
Romney's plan, however, would leave to individual states whether they require all residents to have insurance, as the Massachusetts plan calls for. The Bay State plan has reduced the number of uninsured by about 300,000 to around 160,000, Canfield said. Romney also supports full tax deductibility of all medical expenses, including insurance premiums.
Senator John McCain of Arizona advocates deregulation to allow licensing of doctors and insurers across state lines and eliminating "the bias toward employer-sponsored health insurance." McCain would create a refundable tax credit of $2,500 for individuals and $5,000 for families who purchase their own health coverage.
To pay for the credit, which would come dollar for dollar off the income tax to offset insurance premiums, McCain would phase in a system that would make employer contributions to health coverage a taxable benefit, said Douglas Holtz-Eakin, McCain's senior policy adviser and a former director of the Congressional Budget Office.
McCain would also support a lump-sum payment of Medicare funds to hospitals and doctors to treat certain conditions to reduce duplication and bureaucracy. .
Former New York City mayor Rudy Giuliani has proposed an income tax deduction of $7,500 for individuals and $15,000 for families to create incentives to buy private health insurance. Giuliani also calls for an insurance tax credit for lower-income Americans not eligible for Medicaid, and a cap on medical malpractice awards.
Former Arkansas governor Mike Huckabee proposes full tax deductibility for health insurance costs for individuals and families, tax credits for lower-income families, and promotion of preventive programs to reduce costs for treatment of chronic illnesses.
Former senator Fred Thompson's website describes his general support for better "prevention, chronic-care manager, and personal responsibility," more information technology, less regulation, and the promotion of medical research life-sciences innovation. .
Representative Ron Paul calls the US healthcare system "a federally mandated disaster" and advocates tax deductibility of all medical expenses and making every American eligible for tax-free health savings accounts.
---------
"Uninsured Mass. residents face monthly fines starting in January"
By Steve LeBlanc, Associated Press Writer, December 24, 2007
BOSTON --Come Jan. 1, Massachusetts residents who still haven't signed up for health insurance will start racking up fines on a monthly basis.
Those penalties may be up to half of the monthly premiums for the least expensive health care plan available, although the exact amount of the fines is expected to be announced as soon as this week.
That's on top of the loss of the $219 personal tax exemption for anyone not insured by the end of December.
The fines are part of an increasingly more aggressive approach written into the state's landmark health care law designed to pressure Massachusetts residents into getting insurance. The law, intended to create near-universal coverage in the state, was approved by lawmakers and signed by former Gov. Mitt Romney in 2006.
Even those residents who already have insurance will see some changes when they file their taxes this year.
Everyone, including those insured through their employers, will be required to fill out a new tax form proving they have insurance to avoid paying penalties.
That form -- dubbed 1099-HC -- will require taxpayers to provide the name of their insurer and their subscriber number.
The form will also allow individuals and families to claim an exemption to the law -- either for religious or hardship reasons. Those claiming exemptions will be asked to provide supporting information to back up their claim.
Those who still refuse to get insurance even after being deemed able to afford it, will see the penalties add up quickly.
The monthly premium for the least expensive health care plan -- a so-called "bronze level" plan with no prescription drug coverage -- for a 37-year-old male living in Boston is $196.
Under the law, the penalty for not getting insurance could be up to half that cost -- about $98 a month, or $1,176 for the year.
The actual penalty will be determined by the Department of Revenue that is charged with coming up with the fine structure.
A spokesman for the department said the goal is to keep the fines as simple and clear as possible so everyone knows the cost of not getting insurance.
"It will be a dollar amount so it will be clear," department spokesman Bob Bliss said. "We will try to keep it as simple as possible so people can understand it."
Bliss said the department launched an outreach campaign this year to alert people to the new law, including mailing postcards and distributing flyers to taxpayers, setting up a web site and creating a video tutorial to walk taxpayers through the new form.
Health care advocates have also worked hard canvassing neighborhoods and teaching people about the law which provides free or subsidized care for people making up to three times the federal poverty level.
They say the state should go easy on the monthly fines next year.
"We'd like to see those penalties be as least harmful as possible for families who are trying to put this together and trying to comply with the law as best they can," said Lisa Vinikoor, an organizer with the Greater Boston Interfaith Organization. "This is all brand new."
No one knows for sure how many taxpayers will face the loss of their personal exemption or the monthly fees.
Those charged with overseeing the law have celebrated what they said will be the addition of about 300,000 Massachusetts residents to the ranks of the insured this year -- largely as a result of the law.
But no one can say how many uninsured remain.
Earlier this month, Leslie Kirwan, Gov. Deval Patrick's top budget chief and chairwoman of the Connector board, said estimates of the number of uninsured in Massachusetts before the law took effect ranged from 370,000 to more than half a million.
Bliss said officials will have a much better idea as people begin to file their taxes and are forced to say whether they are insured or not.
--
On the Net:
The Massachusetts Department of Revenue: www.mass.gov/dor
The Massachusetts Commonwealth Health Insurance Connector: www.mahealthconnector.org
---------
"Prison healthcare costs outpace California inmate population"
By Jordan Rau, Los Angeles Times, December 28, 2007
SACRAMENTO - When a judge put Robert Sillen in charge of healthcare in California prisons, the medical staff was vastly underpaid. Software used to track the medical histories of inmates could not transfer information between computers.
San Quentin State Prison had only one phone line for incoming calls and none to dial out, isolating doctors who needed to talk to specialists and other professionals.
"It's just shameful what the state has done," Sillen said in an interview.
He has been trying to fix things, but solutions come at a price: Healthcare spending in state prisons has doubled in the last two years. Sillen's court-ordered intervention is just one reason California's prison spending has far outpaced the swelling number of inmates, contributing to the state's projected $14 billion budget gap, which would be the worst since Governor Arnold Schwarzenegger's election in 2003.
The prison population has grown by 8 percent since then, to more than 173,000 inmates. But the Department of Corrections and Rehabilitation's budget has exploded by 79 percent to $8.5 billion and is expected to top $10 billion next year.
Prison spending is greater than that of any other major program except public schools and healthcare for the poor. The nonpartisan legislative analyst's office projects 6 percent annual increases in prison spending for the next five years as a new prison and dozens of building additions are constructed and opened.
The causes of the department's fiscal metastasis are the same ones that plague many parts of California's $145 billion state budget: spending set at the ballot box and in the courts; bureaucratic waste, failed efforts to help inmates stay away from crime after their release; and more than a decade of neglect in construction, repairs, and other improvements.
.
Voters, too, have contributed to the burgeoning budget, notably by approving the "three strikes" initiative in 1994 authorizing life imprisonment for repeat felons and "Jessica's Law" in November 2006. The latter measure restricts where released sex offenders can live and requires that they be tracked by satellite for life.
Over time, the cost of tracking paroled offenders could grow to $100 million or more, the state says.
Another initiative is being readied for the ballot next year by the authors of last year's measure: Sharon and George Runner, two Republican lawmakers from Lancaster. The proposed initiative would require the state to spend nearly $1 billion to combat gang crimes and lengthen some prison sentences.
"People are trying to do one-upmanship to claim, 'I'm tough on crime,' and it has a cost to it," said Senator Mike Machado, a Democrat who oversees the corrections portion of the state budget.
A report by the inspector general in February found that the corrections department repeatedly failed to correct problems that had been identified in studies the department commissioned.
Department officials admitted this month that as many as 33,000 prisoners might be scheduled to remain behind bars longer than they were supposed to because corrections officials miscalculated their sentences. The longer stays could be costing the state nearly $26 million extra each year.
There is little sign that the growth in the prisons budget will abate any time soon. Prison healthcare spending has increased 263 percent since 2000, to $2.1 billion a year, and Sillen predicted that he would raise it by as much as $500 million for the fiscal year that begins in July.
---------
(A Boston) GLOBE EDITORIAL
"The cost of no coverage"
December 29, 2007
THE EFFORT to give all Americans health insurance has been going on for generations, so far in vain. But the need remains as urgent as ever, and a study by the American Cancer Society ought to cause advocates to redouble their efforts to provide this essential protection.
The study, which appears in a journal published by the society, focused on lung, colorectal, and prostate cancers in men, and breast and colorectal cancer in women - all among the top causes of cancer deaths. The study provides evidence for an obvious conclusion: Those who are without insurance don't benefit much from advances in cancer care that are predicated on early discovery and treatment.
"Lack of health insurance, even for intermittent periods, is associated with lower likelihood of having a 'medical home,' or usual source of healthcare," the study concluded. People in Massachusetts should be proud that their state has pioneered a system in which everyone is required to obtain health insurance, with those at lower-income levels receiving subsidies from the state. Many healthcare advocates would prefer one in which the state provides insurance for everybody, but at least the Massachusetts arrangement pushes residents into finding the "medical home" that might save their lives - a breakthrough in universal coverage.
People on Medicaid, the federal/state system for poor Americans, do not have as high survival rates as those with employer-sponsored insurance. That's no surprise to the researchers who did the study. Many people become eligible for Medicaid only after they become too sick to work; by then they have less chance to benefit from cancer treatment.
African-Americans with insurance had worse outcomes than white patients with insurance. But the study found that for breast and colorectal cancers, the survival rate after five years was still better for those of whatever race who had private insurance than those who were on Medicaid or did not have coverage. Public-health workers need to do a better job of getting out the word about testing and cancer prevention to members of minority groups. But this nation also has to make sure that every citizen has health insurance.
After the study was released last week, the Associated Press estimated that 20,000 uninsured people died of cancer in 2005. That's only 4 percent of the total. Terminal cancer is in most cases an affliction of the old, and almost all Americans 65 years or older are protected by Medicare. Cancer may still kill them, but they are guaranteed through Medicare an opportunity to get the treatment that may prolong their lives. All Americans should enjoy this protection.
---------
"Penalties to rise for shunning insurance: State healthcare levy could exceed $900"
By Jeffrey Krasner, (Boston) Globe Staff, January 1, 2008
Penalties for Massachusetts residents who can afford health insurance but do not purchase it in 2008 could quadruple compared with the maximum penalty in 2007, according to draft regulations released by the Department of Revenue yesterday.
The maximum penalty for those who flout the law and do not buy health insurance would be $912 a year, compared to $219 in 2007.
The higher penalty is intended to get those who are on the fence to buy health insurance. For those wavering, it could make more sense to pay for insurance than to pay the penalty.
The proposed penalties also drive home the full impact of the health reform law's personal mandate principle. This approach makes buying health insurance a responsibility of all residents, similar to the way drivers are required to purchase auto insurance. The penalty was enacted to spur residents to purchase insurance rather than rely on the care hospitals are still required to provide to patients regardless of coverage or ability to pay.
"We have worked hard to craft these penalties in a manner that is straightforward and easy to understand," said revenue commissioner Henry Dormitzer in a statement. "We hope they will encourage people who can afford health insurance to buy it."
In a statement explaining the penalties, the revenue department said, "These penalties apply only to adults who are deemed able to afford health insurance."
Residents who cannot afford insurance, based on state standards, won't be penalized. Residents who face penalties can appeal.
Residents can comment on the proposed penalties until Jan. 15. The regulations will be finalized early this year. Residents won't face the proposed penalties until early 2009, when they file their tax returns for 2008.
The health reform law, signed by former governor Mitt Romney in April 2006, states that the penalty for 2007 would be the loss of an individual's personal income tax exemption. This will cost residents who didn't get coverage $219 when they file their 2007 state income tax return.
Under the law, penalties for 2008 and beyond would be tied to the lowest-cost option of insurance coverage. But it was up to the revenue department to determine the precise formula.
Under the formula issued yesterday, the amount an uninsured resident pays for 2008 varies by income and how long the resident goes without insurance. For instance, those 26 and younger who earn too much to qualify for low-cost insurance and who go the whole year without coverage would pay a $672 penalty. Those 27 and older would pay $912, the maximum. Those who have coverage for part of the year would pay a corresponding amount of the penalty.
In addition, those who earn less than 150 percent of the federal poverty level, or $15,324 for an individual, won't face penalty.
The fees are based on half the cost of the least expensive insurance plan available to each resident but are capped to avoid excessive fees. Thus, a 60-year-old resident of Boston, who would pay more than $4,600 a year for health insurance provided by the state, could have been hit with a $2,300 penalty. But the maximum possible penalty is $912 for all residents. The draft regulations are available at the revenue department's website at mass.gov/dor.
It is still unknown how many residents will have to pay the $219 penalty for 2007, according to the Department of Revenue and the Massachusetts Health Insurance Connector Authority, which administers the new law. A spokesman for the Department of Revenue, said it would measure how many pay the penalty when 2007 tax returns are filed this spring.
The connector authority has said that about 290,000 residents have signed up for health insurance since the personal mandate went into effect July 1. That includes 160,000 residents who qualify for subsidized coverage, 70,000 who qualify for Medicaid, the government health plan for the poor, and 60,000 who purchased full-cost coverage through the state or their employers. The tally will be updated Jan. 10.
Before the health law was implemented, the state estimated that about 400,000 residents lacked health insurance while the US census estimated the number of uninsured was 657,000.
John E. McDonough, executive director of Health Care for All, an advocacy group that helped craft the health insurance law, said he was pleased with the proposed penalties.
The department "really listened, and we see a lot of our concerns reflected in this schedule," said McDonough. "It's fair, simple, and sensitive to the needs of residents."
-
Jeffrey Krasner can be reached at krasner@globe.com.
-----
Henry Dormitzer Joins Free Flow Power as CFO
Free Flow Power Corporation announced today that Henry Dormitzer, currently Governor Deval Patrick's Commissioner of Revenue for the Commonwealth of Massachusetts, will join the Company as its Chief Financial Officer on February 4, 2008. Mr. Dormitzer will be responsible for raising $3 billion for hydrokinetic energy projects on the Mississippi River to be developed by Free Flow Power, a clean renewable energy company.
Gloucester, MA (PRWEB) January 5, 2008 -- Free Flow Power Corporation announced today that Henry Dormitzer will join the Company as its Chief Financial Officer on February 4, 2008. Mr. Dormitzer is currently the Commissioner of Revenue for the Commonwealth of Massachusetts where he manages the Department of Revenue's staff of 2,300 public employees and is responsible for administering the state's tax laws, enforcing child support obligations, overseeing local budgets, and implementing parts of the state's new health care reform law. Mr. Dormitzer has also been central to Governor Deval Patrick's initiative to reform the corporate tax code and lower the corporate tax rate in Massachusetts. He joined the Patrick Administration as Under Secretary for Administration and Finance responsible for capital finance, tax policy, collective bargaining and information technology. Prior to joining the Administration, Mr. Dormitzer spent 15 years as an investment banker with UBS where he was the Managing Director responsible for the firm's Boston office. Mr. Dormitzer is treasurer of the board of trustees of Worcester Academy and has served as a member of the boards of MassDevelopment and the Massachusetts Educational Financing Authority. He is a graduate of Harvard College.
Daniel Irvin, Free Flow Power's CEO said Mr. Dormitzer's responsibilities will include structuring and placing $3 billion of project financing for Free Flow Power's hydrokinetic developments on the Mississippi River. "Henry has vast capital markets experience financing complex projects, strategic vision, serious management experience and genuine integrity. We want all of our senior mangers to be someone who can run the Company tomorrow, and Henry fits that description."
Free Flow Power is a leading hydrokinetic project development and turbine manufacturing company engaged in producing clean, renewable energy from moving water without dams or other adverse environmental impacts. The Company has developed a proprietary magnetic levitation turbine technology that can generate power cost-effectively in free flow environments. Free Flow Power is focusing on developing sites in major rivers, but its technology is also applicable to tidal and current energy. The company is also actively marketing its turbine technology to other developers of hydrokinetic projects and owners of existing dams and other infrastructure.
-
Source: www.prweb.com/releases/2008/1/prweb602152.htm
-
Company web-page: www.free-flow-power.com
-
---------
"Long-term care insurance on rise"
By Ellen G. Lahr, Berkshire Eagle Staff
Friday, January 04, 2008
Ron and Judy Turbin are among the baby boomers who have witnessed the decline of an elderly relative, whose final years were spent in a nursing home bed.
Judy Turbin's father faded with strokes and dementia, and her mother eventually could no longer care for him alone.
Their finances were modest, so Medicaid covered the cost of her father's nursing home care. He died in 2005, after six years in a Lenox facility.
"Judy's parents were not loaded up with resources, and so his was a clear-cut Medicaid case," said Ron Turbin, a semi-retired lawyer and Williamstown selectman, whose wife recently opened a pastry business. "But we got concerned about our own situation."
Long-term care costs, he said, could be "a financial earthquake, and we might have to sell our house."
The Turbins, who are in their 60s and in fine health, bought a long-term care insurance policy two years ago, for which they spend around $4,000 per year.
"It's worth it, but it's a sacrifice," said Ron Turbin. "Perhaps we have a little less for luxuries, but I really think it's worth it. It's peace of mind."
The policy will pay for nursing home care, but also pays for what Medicaid will not: home care and assisted living.
The Turbins want to ease the potential burden of care on each other and their children, protect their home and assets, and leave something for their three grown children.
Costs on the rise
With the elderly population living longer, their needs for daily help or all-around care are on the rise.
In Massachusetts, average nursing home costs were $270 per day in 2007, according to the National Clearing House for Long Term Care. Assisted living costs an average of about $4,300 monthly, and in-home care runs about $20 per hour.
Unless, and until, the patient is poor enough to meet federal poverty guidelines, nursing home bills must be paid with private funds. That means a potential depletion of savings, retirement funds, home equity, real estate or other assets.
"You can retire with a half-million in the bank, and it can cost $100,000 per year to be in a nursing home," said Gary Kobran, financial services manager of Wheeler & Taylor Insurance in Great Barrington. "But long-term care insurance is a very tough sell. The people who need it most are the middle class, not poor, not rich."
Those who do buy are getting younger, however, according to Jackie Metsma, a financial planner and long-term care insurance specialist for True North Financial Services, based in Williamstown.
"People used to look at this option when they prepared to retire, but now more people are in their early 50s," she said. "People are now going through things with their parents, and they don't want their own kids to go through it."
The American Association of Retired Persons estimated in 2005 that 7 million long-term care policies were in place, with the typical consumer at age 61.
Nearly half of those policy holders had incomes above $75,000 per year and more than $100,000 in liquid assets.
In 2005, the average annual insurance premium, across all age groups, was $2,000, according to the federal government's data.
Industry changes allow discounts for couples, and some companies sell "hybrid" policies that combine long-term care insurance with life or disability insurance, said Metsma.
Sharp hikes
The earliest policies written have taken sharp price hikes in recent years.
George and Caroline Farley, of Pittsfield — he is 81, and she is 77 — bought policies 14 years ago through their son, Shaun Farley, a broker now with Greylock Insurance.
The Farleys' initial annual premiums were $1,700 for him, and $1,100 for her, said George Farley, a retired schoolteacher.
But their most recent bill was a shocker: $3,700 for him, and $2,700 for her.
Though the policy cost has spiked, he said, "we will stick with it. We don't want to lose it."
They also want to live at home as long as possible, he said.
Kobran, of Wheeler & Taylor, said the Farleys are victims of the insurance industry's early errors in financial projections.
The insurance industry, which is closely regulated, relies on income from interest earnings to pay claims, and interest rates have been low in the 20 years since long-term care insurance has been around.
Second, insurance companies assumed a higher number of policies would lapse through non-payment. That, too, proved incorrect, he said.
Most people with long-term care insurance keep it.
Patrick Sheehan, of Sheehan Health Group, which owns Craneville Place nursing home and Sugar Hill Assisted Living, said many people who have purchased long-term care insurance have not yet reached the age of needing the benefit.
Those people who do have it, he said, tend to use it for assisted living, but the numbers remain relatively small.
He advised that anyone seeking long-term care insurance become an educated consumer, since benefits vary widely, he said.
"Be smart consumers; use caution," he said. "You really need to shop around, make sure you're getting the best value for your money."
At a glance ...
Average costs in Massachusetts for long-term care
Semi-private nursing home room: $270/day
Assisted living facility: $4,300/month *
Home health aide: $20/hour * * Not covered by Medicaid
Tips for shopping for long-term care insurance:
Don't buy long-term care insurance out of fear or emotion.
Consult a certified financial planner to determine whether your money should be used on long-term care insurance.
Consult an insurance broker who has access to a wide variety of potential underwriters.
Consider benefit options: Do you want full, comprehensive coverage, and can you afford it? Do you want a lifetime benefit, or a five-year cap?
Can you tailor a less comprehensive plan that provides partial coverage, which you can supplement with income from assets or other funds?
Do you want a 'hybrid' policy, which combines life insurance or disability insurance with long-term care coverage?
Do you have a pre-existing condition? People already in need of long-term care services won't qualify.
SOURCES: American Association for Retired Persons; National Clearinghouse for Long Term Care Information
---------
"Costs a big concern for health care"
By Steve LeBlanc, Associated Press
Monday, January 7, 2008
BOSTON (AP) — Massachusetts is facing a daunting goal as it enters the second year of its grand experiment of extending health care coverage to nearly all citizens — reining in spiraling costs that could threaten the landmark law.
"The sustainability of reform depends on our ability to restrain or constrain or moderate the increase in costs," said Jon Kingsdale, executive director of the Health Insurance Connector Authority, which oversees the health care law.
"That's going to take a huge concerted effort by all players in the health care area," he added.
For Massachusetts residents deemed able to afford health care, but refuse, that means facing new monthly fines that could total as much as $912 for individuals and $1,824 for couples by the end of the year.
That's a steep increase. Those who failed to get insured in 2007, the first year of the law, faced the loss of their personal exemption on their tax returns, worth $219.
But pressuring individuals to get insured is only part of a multi-pronged attempt to cut health care costs to ensure the viability of the law, which has thrust Massachusetts into the center of the national healthcare debate.
The state's insurers, hospitals and lawmakers are also finding themselves under pressure to slow spending, or come up with new revenue.
Much of that pressure is being felt by hospitals.
"Hospitals are probably the largest perceived target because they are easy to identify," said Lynn Nicholas, president and CEO of the Massachusetts Hospital Association.
The state's hospitals are pursuing a series of initiatives to help slow rising costs, from streamlining administrative functions to bringing on more qualified health care workers, especially nurses, Nicholas said.
Hospitals are also looking at the way they manage chronic diseases to see if they can improve care while trimming costs. They are beginning with diabetes, a disease that disproportionately affects minorities and can lead to more serious health problems.
"We can deliver better care to people with diabetes and we can do that in a way that at the same time reduces the cost of care," Nicholas said.
The state's insurers also say they are committed to reducing costs.
Dr. Marylou Buyse, president of the Massachusetts Association of Health Plans, said the group has unveiled its own cost-cutting plan and called for public hearings to study the issue.
"We have to understand what is driving the rising costs because unless you understand the problem, you can't come up with solutions," she said.
Kingsdale said the health care community should look at a range of options.
One strategy is to institute new safeguards to reduce medical errors, he said. That could shorten the length of hospital stays and cut down on the number of readmissions, all factors driving up costs.
Kingsdale also said limiting reliance of expensive tests — like CT or MRI scans — when they are of questionable medical help could also cut costs without hurting the quality of care.
Officials also need to consider limiting the cost of a day in the hospital and cutting administrative costs, he said.
"It's probably going to be a combination of all of those," he said.
No one is expecting costs to drop. Kingsdale said his goal is to limit annual cost increases to about five percent for the state's $60 billion health care industry. That's compared to recent double digit increases.
The state also needs to be prepared to step in with more money if needed, although Kingsdale said he has "no idea how much more the state is going to have to put in."
No one knows for sure exactly how many residents remain uninsured despite the enormous effort of the last year. Estimates before the law took effect ranged from 400,000 to 600,000.
During 2007, the state enrolled about 300,000 of those, whether in subsidized programs or in lower-cost non-subsidized plans.
Kingsdale that the state has to stand firm on the most controversial part of the law, the requirement that those who can afford insurance be required to pay for it. The state makes free or discounted insurance available to poor and low income residents.
"In 2008 it's a more substantial penalty and it will probably go up again in 2009," he said. "The intention is not to penalize people, but to motivate them to get enrolled."
While some health care advocates say they are waiting to see the impact of the higher fines on individuals and families, hospital association CEO Nicholas said she agreed the state has to stand firm.
"One of the biggest pressures is will we have the ability to stick to our guns on personal responsibility?" Nicholas said. "If we get soft on that issue everything could go down."
---------
"Healthcare spending rises 6.7%: Drug purchases up as Medicare plan eases access"
By Associated Press, January 8, 2008
WASHINGTON - Seniors and the disabled flocked to the pharmacy counter in 2006 with their new Medicare drug cards, fueling a 6.7 percent increase in health spending, the federal government reported yesterday.
In most other areas of healthcare, there was a welcome slowdown in spending. It still cost more to go to the hospital or doctor, but the increase was not as great as in the previous year.
The $2.1 trillion spent on healthcare in 2006 came to an average of $7,026 a person. Healthcare represents 16.1 percent of the economy. The increase in drug spending occurred even as consumers relied more on generic drugs and as prices remained relatively stable for many brand names. Nearly two out of every three prescriptions filled were generics, which helped restrain drug expenditures.
But that restraint was offset by the new Medicare benefit. Those with insurance are more likely to access the healthcare system. Under the drug benefit, people who once had to forgo or cut back on medicine had the means to fill more prescriptions in 2006, thanks to the new government subsidy.
Also, under the drug benefit, many of the poorest beneficiaries were moved from Medicaid into Medicare, where private plans administer the drug benefit. Those private plans failed to negotiate discounts as large as those that the states got. Officials said the discounts drug manufacturers were required to give states typically lowered costs about 30 percent. Meanwhile, the private plans typically negotiated discounts of 5 to 10 percent. Spending on prescription drugs increased 8.5 percent in the drug benefit's first year - compared to 5.8 percent the year before.
Overall, healthcare makes up a growing share of the nation's economy - a trend that many analysts worry will eventually harm the economy as businesses, the government, and consumers have to divert resources from other priorities to pay health bills.
"Costs continue to grow faster than income, and there's no reason to believe this won't continue," said Paul Ginsburg, president of the Center for Studying Health System Change, a research organization.
Ginsburg said the government and private sector is not helpless when it comes to lowering health bills. Medicare and the private sector can put more emphasis on encouraging healthy lifestyles and reducing obesity rates, he said. They can also focus their payments so that there is not such a huge incentive for doctors to order extra tests, imaging scans, and various other procedures.
The report by economists from the Centers for Medicare and Medicaid Services, published in the journal Health Affairs, showed that spending on:
Home healthcare rose 9.9 percent in 2006. In each of the previous two years, home health spending increased 12.3 percent.
Nursing home care rose 3.5 percent.
Wheelchairs, walkers, artificial limbs, and other such medical equipment rose 2.3 percent.
Spending on hospitals and physician services accounts for about half of each dollar spent on healthcare in the United States. Spending for both slowed slightly in 2006. Spending rose 7 percent for hospital care - versus 7.3 percent the year before. Spending for physician services rose 5.9 percent - versus 7.4 percent the year before.
---------
Berkshire County, Massachusetts
"Shortage looms in primary care: Berkshire docs are 'feeling beaten down' and many plan to leave their practices"
By Jack Dew, Berkshire Eagle Staff
Monday, January 07, 2008
Nearly half of Berkshire County's primary care doctors are dissatisfied with their practice, according to a new survey, mirroring statewide and national trends that suggest a looming shortage.
A committee of Berkshire primary care doctors, working with the Massachusetts chapter of the American College of Physicians, surveyed their peers throughout the county and found that 46 percent said they were dissatisfied with their practice.
The committee — led by Dr. Robert Jandl of Williamstown — sent the survey to all 79 internists and family practitioners who serve as primary care providers for adult patients in Berkshire County. Sixty-nine — or 87 percent — responded.
Of that number, 46 percent said they had reduced their clinical hours or were planning to leave the field. And 63 percent said they probably or definitely would not enter primary care again, while 91 percent said they would have reservations or recommend against others going into primary care.
Jandl summarizes the findings in a column on today's Commentary page, where there also appears a statement signed by 49 local primary care doctors urging reform of the medical system.
The survey results are similar to the statewide and national mood, where primary care has increasingly become an unpopular specialty. Fewer medical students are pursuing primary care, opting for better-paying, procedure-based specialties, studies have shown. Meanwhile, the Massachusetts Medical Society found that 60 percent of doctors surveyed statewide said there are not enough internal medicine providers in their community, and 27 percent cited a lack of family-practice physicians. Those two specialties represent almost all primary care doctors.
Dr. Dale Magee, president of the Massachusetts Medical Society, said primary care doctors are being paid less and asked to do more while their role in the health care system is being denigrated.
"They feel beaten down, asked to do more with less and, as a result, are feeling very downtrodden," Magee said.
Reaffirming fears
In an interview, Jandl said the Berkshire County survey results reaffirmed his fears about the state of primary care. "When you are actually looking at the hard data, it can have a riveting effect, and I hope it will have a motivating effect on others to realize how grave the situation is."
The survey began with a list of 165 doctors that the state Board of Registration in Medicine believed to be practicing primary care in the county. But the committee found that many of those physicians were specialists, worked in emergency departments or had retired.
Of the remaining 79 doctors, 66 percent said they have had difficulty finding qualified primary care doctors to join their practices.
In interviews, doctors said the treatment climate is spoiled by insurance companies that micromanage care and oversee a reimbursement system that pays primary care providers the lowest rates of all specialties. Although doctors are earning less, they have to spend more on office staff to cope with the ever-increasing paperwork.
"I love doing this," said Dr. Andrew Schamess of Lenox, "but sometimes I feel so deeply discouraged when I read the latest thing the insurance companies are up to, how much more paperwork they can dump on us, how much more they can cut our fees."
Schamess said the "joy of primary care — and the greatest benefit to the patient — is being able to spend time with patients. The best primary care physicians are the ones who take their time and listen and take every problem seriously and try to solve it. That is becoming harder and harder to do."
Subtle yet powerful
In the quest to control costs, insurance companies have increasingly tried to insert themselves into the doctor-patient relationship, Jandl said, sometimes in subtle yet powerful ways.
For example, by requiring patients to pay more for one drug than another, the companies drive their clients to the cheaper drug. The patient calls his doctor and asks that his prescription be changed. The insurer "has just created an administrative task for me that has zero value in patient care," Jandl said. The drug may interact poorly with another drug or may not be as effective. And then there are the headaches of getting the paperwork to the insurer and the pharmacy. "It creates a whole storm of administrative work."
Dr. Charles Wohl in Pittsfield said the lot of primary care doctors will not improve substantially unless the health care system improves; he advocates adopting universal health care.
"We are trying to deliver good health care in a highly dysfunctional health care system," Wohl said. "For primary care providers, reimbursement for the amount of time we spend is very low. We spend at least 20 percent of our day on uncompensated work ... doing the things we are supposed to do. The result is that offices are not earning the revenue they need without increasing the number of patients that they see, which means decreasing the amount of time with each patient."
Although an array of reforms could improve their position, doctors interviewed cautioned that each would require systemic change. For now, the Berkshire committee is hoping to call attention to what it describes as a dire situation.
"We are being forced to represent insurance companies' interests in our interactions with patients. That corrodes trust," Jandl said. "I am hoping, through these efforts, to illustrate that (doctors and patients) want the same thing, and we shouldn't be at odds with each other. We all want to get and deliver competent, personalized, highly valued and skilled care."
-
To reach Jack Dew: jdew@berkshireeagle.com, (413) 496-6241
--
"Chasing out the doctors"
The Berkshire Eagle - Editorial
Wednesday, January 09, 2008
The dissatisfaction of Berkshire County's primary care physicians, which mirrors that of their counterparts across the state and nation, is a product of a health care system run not by physicians but by health insurance paper-pushers. The system conspires against both doctors and patients, and is a mystery to the rest of the civilized world, where excellent, inexpensive care and patient and doctor satisfaction are the rules, not the exceptions.
A committee of primary care doctors led by Dr. Richard Jandl of Williamstown surveyed the county's 79 internists and family practitioners who serve as primary care providers, 87 percent of whom responded, and found that 46 percent were dissatisfied with their practice. That same percentage indicated that they had reduced their clinical hours or were planning to leave the profession, and 91 percent said they would have reservations about recommending the field to others. Berkshire County may be facing not only the loss of its primary care doctors in the years ahead but the grim reality that they are irreplaceable, at least by doctors of comparable skill.
Primary care physicians comprise the first line of defense in the health care industry, as they consider the total wellness of the patient and get to know the patient over a period of years. They are the main advocates of preventative medicine, which enables patients to avoid the kind of expensive ailments that can devastate bank accounts while jacking up the cost of health insurance. Unfortunately, the insurance industry is working actively to make the lives of primary care doctors miserable.
Preventative care, which is a priority in nations with national health care, is discouraged by the many insurers who provide less and less financial coverage for check-ups and examinations, such as routine breast examinations for women. Many insurers are questioning the need for the yearly physical, a medical practice that enables doctors to catch minor problems before they become major ones. These are the kinds of decisions that should be made by trained medical professionals, not insurance company bureaucrats looking to pad the bottom line to please shareholders or win bigger bonuses for overpaid CEOs.
Primary care physicians are paid the lowest of all specialties because of the insurance industry's low regard for them. This encourages them to leave the field and discourages other doctors from entering it. Insurance companies dump red tape on physicians, reducing patient time and requiring doctors to hire large staffs to cope with the paperwork. While drug companies push their products on national television, insurance companies direct patients to cheaper generics, creating patient dissatisfaction that falls onto the primary care doctors. Not only is it understandable that so many family physicians have left the field, it is a tribute to their dedication to medicine and their patients that so many remain.
In a statement on Monday's opinion page accompanying a column by Dr. Jandl, 49 Berkshire primary care physicians advocated "dramatic and fundamental reform." Introduction of government-run, single-payer health care would bring about that reform by getting the insurance companies out of the equation, but with deep-pocketed insurance lobbyists filling the campaign coffers of Washington officials, single-payer has gotten nowhere.
There are, however, winds of change blowing this election season. Democratic presidential candidate Barack Obama, perhaps the leading "agent of change" to emerge so far, has endorsed single-payer, but with the disqualifying proviso that the system remain employer-based. No system that continues to burden employers and employees with punishing health care costs can be defined as reform.
How bad does it have to get in America before major health care reform is instituted? Let's hope that dedicated and needlessly burdened Berkshire primary care physicians and their patients don't have to wait to find out.
---------
"What's wrong with health care?"
The North Adams Transcript - Letters
Thursday, January 10, 2008
To the Editor:
A report issued by the World Health Organization indicated that the U.S. health system spends a higher portion of its gross domestic product than any other country, but ranks 37th out of 191 countries acording to its performance. France, Italy, Spain, Austria and Japan have health care systems that surpass ours. Even more embarrassing is that several smaller countries like San Marino, Andorra, Malta and Singapore outrank us as well.
Recently I had first-hand experience with the U.S. health care system and found it to be sorely lacking. The story by its nature is anecdotal, but it is highly representative of the problems in our health care system.
I was scheduled to have knee replacement surgery. Prior to surgery, I conditioned myself for the recovery period. I lost a substantial amount of weight and exercised five to six days a week, thus increasing my lean muscle tissue and strength and stamina. I was told to expect a five-day hospital stay followed by one to three weeks in a rehabilitation facility.
The surgery was completed with due credit to the surgeon's capabilities. I walked on the leg less than 24 hours after surgery. All seemed to be going well. The case manager stated I would be going straight home instead of rehab. Why? Because I was able to walk 200 feet. I explained that I was a single, disabled senior citizen without a support system. Being able to walk 200 feet was not the same as being strong enough to be on my own. I needed further help.
The case manager informed me in no uncertain terms that this was not the hospital's problem. Since the insurance company would not pay for rehab, they had every right "to put me out on the corner." Yes that is a direct quote. Put me out they did at 5:30 p.m. It was a little after 7 p.m. when I arrived home. I had no food, no analgesia (a prescription, yes) and no means of getting about.
Ten days later, I had my staples out at the orthopedist office at Albany. It was difficult to make transportation arrangements as this was the holiday season and service was pre-booked or offices were closed.
A couple of days later, I noticed a couple of threads pushing through the suture line. My doctor's assistant at Albany said to come right over, but I couldn't make any arrangements. The second suggestion was to have my primary care doctor at North Adams remove them. These sutures were just a couple that had not been absorbed by the body and, if left in, could cause an infection. My primary care doctor would not touch them because the surgery had been done by another physician. Evidently he was concerned more about potential litigation in the event of a problem.
I asked what about infection? I was advised if I got an infection to go to the emergency room and have them removed. Is it any wonder that our ER's are overcrowded and our health care costs are escalating when doctors are encouraging such abuses of the system? Never mind thinking about the increase pain and suffering to the patient.
It has been a little over three weeks since the surgery. My knee, leg and hip are painful. I had to go to the ER for this pain, to find out the cause and receive treatment. More expenses. The physical therapist assessed that the aggressiveness of my recovery period likely exacerbated the degenerative joint tissue in my hip as well as having strained the ilialatibial band and gluteus media muscles.
So why is the U.S. ranked 37th in health care in the world? Uncaring hospitals, health care workers without compensation, lack of work ethic and pure unadulterated greed. Add into this mix lawyers, politicians, lobbyists and pharmaceutical companies, and we begin to see why we have lost our place as a world health leader.
Beware if you are seeking health care and are elderly, poor, disabled, etc. Assembly line care has already started, and the future of our health care system grows grimmer still.
Maureen O'Brien
North Adams, Massachusetts
Jan. 8, 2008
---------
"A symptom, not a solution"
The Berkshire Eagle - Editorial
Friday, January 11, 2008
With the approval Wednesday by the state Public Health Council of pharmacy-based medical clinics, Massachusetts is moving farther away from needed health care reform. The clinics are the product of a faulty system and will likely contribute to its further decline.
The clinics are designed to improve access to routine care and lighten the load on emergency rooms, but what they will do is apply a Band-Aid to problems that require major surgery. Patient access is increasingly limited for a variety of reasons, among them high health insurance costs and the dwindling number of frustrated doctors in the primary care field (Eagle, Jan. 7). Emergency rooms are crowded for those reasons, as well as health insurer indifference to preventative medicine.
CVS Corporation is poised to open more than two dozen of these clinics, and this move into for-profit medicine raises questions of its own. Will these clinics put a further squeeze on already struggling independent pharmacies? Almost assuredly. Is episodic health care at a clinic the equivalent of the care given a physician who knows a patient's medical history? No. Is the state prepared to conduct oversight of these clinics? There is no reason to believe so.
The clinics are not the solution to a problem but the symptom of a larger one — a health care system that grows worse with attempts like this one to patch its faults.
---------
The Berkshire Eagle - Op-Ed
"Put docs before executives"
By Susanne L. King, M.D.
Wednesday, January 16, 2008
LENOX, Massachusetts
Last week, The Berkshire Eagle published several articles about the crisis in primary care in our county. This crisis should be of concern to everyone because primary care is the bedrock of our health care system. There is already a shortage of primary care doctors, and those currently in practice in Berkshire County are having difficulty recruiting new physicians to their practices. One-third of the existing primary care doctors in the county will retire in the next 10 years. An aging population has increased the need for primary care doctors, and this makes the shortage even more dire.
Unfortunately, the crisis is not addressed by the current Massachusetts health care reform legislation (Chapter 58). By focusing simply on having health insurance mandated for everyone, the legislation does not address (1) the lack of affordability of insurance premiums for many individuals, (2) the lack of access to care when an underinsured individual can't afford to pay the co-payments or deductibles when he needs to use his insurance, (3) the lack of affordability for the state in subsidizing many of the insurance premiums, (4) the lack of any mechanisms for controlling the increase in costs of health care, (5) increasing administrative burdens for doctors, (6) increasing costs for businesses, and (7) diminishing coverage as insurance companies slash more and more from benefits in their "innovative insurance products." And we can also add to the list: (8) not addressing the needs of the actual providers of care (like our primary care doctors), who are overworked and underpaid in the current system. The result is diminished access to care for patients.
The solution lies in fundamental reform of the health care system in our state and in our country. We need a single payer health care system, with one administrator of our health care funds, rather than the multiple for-profit insurance companies. Private insurance bureaucracy and paperwork consume 31 percent of every health care dollar. This includes the compensation of CEOs like William Van Faasen, of Blue Cross/Blue Shield of Massachusetts, who earned $16.4 million in retirement benefits in 2006, in addition to almost $3 million in his other role as chairman of the insurance company. If we had a single-payer system, this egregious expenditure of health care dollars would be history.
There is legislation for single-payer health care reform in our state, the Massachusetts Health Care Trust (MHCT), Senate Bill 703. If we had single-payer health care in Massachusetts, it would benefit both physicians and their patients. Primary care doctors would be freed from the administrative burden imposed by the insurance companies: one payer, one claim form.
Primary care would be more valued in a single-payer system. The MHCT legislation specifically addresses the prevention of disease and disability, the role of primary care doctors, as well as the need to increase satisfaction with the health care system among providers and patients. Addressing the issue of 'satisfaction" for doctors and patients is far from the aims and values of the current for-profit health insurance companies. With single-payer health care, patients would be free to choose their own doctors and other health care providers, unlike the current system, which places no value on established doctor-patient relationships, the foundation of primary care.
Since the publication of the articles in the Berkshire Eagle, people have been asking their doctors what they can do to help. Patients can call or write to their legislators, to ask them to support single-payer health care, the Massachusetts Health Care Trust. They can also talk to others about health care reform; a good starting point would be to watch the movie "Sicko," which shows how single-payer health care works in other countries. And patients can write letters to The Berkshire Eagle, as some have already done.
In the final analysis, who do we want to support: our underpaid and overworked primary care doctors who provide our medical care, or insurance company executives like Mr. Van Faasen, who make millions of dollars without taking care of a single patient.
-
Dr. Susanne L. King is a Lenox practitioner.
---------
A Boston GLOBE EDITORIAL
"Easy stop for healthcare"
January 19, 2008
THE MINUTECLINICS that CVS wants to locate in some of its drugstores aren't going to revolutionize healthcare in Massachusetts, but they will be a convenient option for people who need treatment for minor ailments. The state Public Health Council was right to approve them, and the Menino administration should not try to block them from opening in Boston.
The mayor last week contended that the clinics might seriously compromise medical care. "Allowing retailers to make money off of sick people is wrong," he said. By that standard, anybody who sells a cold sufferer a bottle of cough medicine is preying on the diseased. The concept of a MinuteClinic does not pose any ethical challenge as long as the nurse-practitioners at the clinics use their best medical judgment, and do not try to steer patients to products for sale at the CVS store.
Sporadic visits to the clinics would be no substitute for a long-term relationship with a physician, but primary-care doctors are in short supply in Massachusetts. Many people don't have one now, as is evident from by the crowded conditions at hospital emergency rooms during outbreaks of the flu. That illness is usually best treated by staying home and keeping in contact by phone with a physician's office. The clinics will be performing a service for healthcare if they can take pressure off overcrowded, chaotic ERs.
The nurse-practitioner would be limited to treatments of minor conditions as specified in the clinics' licenses. The state Public Health Council, in setting rules for the licenses, made sure that CVS would establish a network of physicians whom the nurses could call if greater medical expertise were necessary. To encourage patients to establish a long-term relationship with a healthcare provider, the clinics will keep a list of local physicians who have openings for new patients. The council insisted that the clinics establish policies to keep the staff from promoting sales at CVS.
These requirements ought to ensure that the clinics offer their limited services without difficulty. The licenses last only two years, and the council can insist on improvements or refuse to renew them if unexpected problems arise.
The mayor also questioned CVS's selling of tobacco, soda, and junk food. But all three are legal products, and it's not reasonable to insist that their sales be curtailed or stopped as a condition for opening a MinuteClinic. The state Public Health Council decided that CVS should post a sign in the clinics saying that tobacco use is harmful, and that warning ought to suffice. The clinics offer too much promise to be derailed by a side issue.
---------
A Boston GLOBE EDITORIAL
"A cavity in children's health"
January 26, 2008
TOOTH DECAY and other dental woes hit low-income and minority children hard, according to a study released this week. It's a public check-up that should push Massachusetts to act.
Children across the country suffer from toothaches and decay, and many go without basic care. In one horrifying case last year, 12-year-old Deamonte Driver of Maryland died because an untreated dental abscess apparently led to a brain infection. His family was poor and frequently homeless.
While most cases aren't this tragic, thousands of disadvantaged children in Massachusetts do suffer from dental pain that hinders eating, learning, and sleeping.
Problems start early. In Massachusetts, 19,000 kindergarteners (28 percent) have tooth decay. And of this number, 10,000 aren't getting treatment, according to estimates in the new report from the Catalyst Institute, a nonprofit that's funded in part by the Delta Dental insurance company. Black children are 1.7 times more likely than white children to be in this group. Hispanic children are 1.8 times more likely. And poor children are almost twice as likely to be in this group as wealthier peers.
There is no one magic cure, but there are ways to weave a stronger dental safety net.
Connecticut sets a good example. It has a statewide oral health plan, which calls for doubling the number of dentists who take Medicaid - by raising reimbursement rates and cutting down on paperwork - and increasing the number of people who get annual dental care. Massachusetts doesn't have such a plan, but it is wisely seeking federal funds to create one. And in the last year, the state has added 200 dental providers who accept Medicaid patients.
Massachusetts already has an Office of Oral Health that's putting up a good fight. The office manages school-based fluoride rinse programs in communities where the water isn't fluoridated. It also promotes the use of dental sealants, a coating to protect against cavities, on children's teeth.
But there's more to do. The state should seek to increase the number of cities and towns that have fluoridated water systems. Currently 139 cities and towns do, including Boston, Somerville, and Cambridge. But most - including Springfield - do not.
Other steps could prove useful. More minority dental students should be recruited to increase diversity and break down some patients' distrust of dentists. And more dental services could be put in schools, public housing, and other alternative settings.
While this state and the nation as a whole have made strides in extending health coverage to poor children, efforts to make sure children have dental care have lagged behind. Massachusetts needs a broad strategy to deal with these needs.
--
"State under court order to boost dental care access"
Boston Globe, Letters, January 29, 2008
YOUR JAN. 26 editorial "A cavity in children's health," while accurately portraying the serious deficiencies in Massachusetts' dental care for low-income children, omits an important fact: Massachusetts has been under a federal court order since 2005 to get its house in order in terms of increasing access to dental care for Medicaid children.
In 2005, as a result of a lawsuit brought against the Romney administration and litigated by the nonprofit law firm Health Law Advocates and Greater Boston Legal Services, a federal court judge found the level of dental care access for Medicaid children "shockingly low," and ordered the state to increase such access under a five-year plan.
At that time, the access level for poor kids in Massachusetts was 33 percent. Three years later, it hovers around 37 percent, hardly dramatic progress. Among those with private dental insurance, the rate of access for kids is about 75 percent. At the current rate of increase in access for Medicaid children, it will take the Commonwealth until 2034 to provide access for at least 70 percent of Medicaid children.
The Commonwealth needs to act decisively to attract dentists to the Medicaid program and to take other necessary steps to comply with the court's order.
BARBARA ANTHONY
Executive director
Health Law Advocates
Boston, Massachusetts
---------
Stretching benefits
Companies offer yoga as perk, curb on health costs
By Kristi Ceccarossi, Boston Globe Correspondent, January 26, 2008
CAMBRIDGE - For most of the workweek, Dong Li is shackled to her desk, a sedentary hostage to project deadlines, dressed in crisp business casual, and suffering an increasingly stiff neck.
But for at least two hours, Li, a senior program analyst at Abt Associates, a research and consulting firm, is liberated.
Barefoot and in sweats, every Monday and Thursday during lunch hour, she bends, breathes, and stretches on the industrial carpet in Abt's basement alongside a dozen or so of her co-workers.
The ancient Indian tradition of yoga has quietly become a $3 billion a year business nationwide, and has made significant inroads in corporate America.
At Abt, corporate yoga is a benefit offered to the company's 400 workers. For $6, employees can take a class. Abt provides the space, picks up the other half of the tab, and hires Diane Dymek, a certified instructor who operates Begin Within Yoga, of Waltham, to teach.
"I look forward to Mondays because of it," Li said.
Over the last 20 years, many employers have developed wellness benefits as a way to stave off rising insurance costs by improving worker health. Generally, they include discounted gym memberships, diet groups, or smoking-cessation courses.
But in recent years, many Massachusetts companies, including Stride Rite Corp., Tufts Health Plan, and Dunkin' Brands Inc., have incorporated yoga into the workweek.
It can be an odd fit, given that yogic philosophy emphasizes relaxation, peace, and spiritual oneness, not exactly the mantras of the corporate world. But benefits coordinators say the practice of meditation and balance is useful in the workplace.
"Yoga has helped people take a step back and look at a problem from a different angle," said Patricia McIntyre, who heads the wellness program at Abt.
While the benefit of corporate yoga for employees is a subjective matter, the benefits for yoga instructors dozens of whom are graduating from Boston-area studios each year are undeniable.
According to Toby Kumin, co-owner of Boston Yoga, an online business directory, there are more than 40 studios in and around the city. Despite the $500,000 to $1 million cost to get a studio off the ground, new practices are opening regularly and existing studios are growing, she said. This month South Boston got its first studio, Somerville-based O2 expanded to the South End, and Prana Power Yoga, in Newton, opened a Cambridge location. Prana plans another in Winchester next month.
But, Kumin said, a lot of studio owners can't rely on class fees alone to pay the bills. Corporate yoga, which she also practices, is a reliable supplement. Dymek, whose entire livelihood is generated by her corporate yoga practice, said she earns about $1,000 a week. "It's really the only way to make an income doing yoga," she said.
Practitioners say healthier, happier employees are more productive. On that premise, starting as early as the 1980s, wellness advocates began introducing physical activities into the workplace. But it wasn't until advocates could start selling wellness as a way to improve the bottom line that fitness centers and weight loss programs became a mainstay at large corporations.
"For years we had to talk companies into this idea," said Iris Sokol, owner of Fitness Works at Work, a wellness-management firm in Sherborn that works with Genzyme Corp., Papa Gino's Inc., and Dunkin' Brands. "Now, not a week goes by that we don't get a phone call from an employer who wants to bring us in."
As of 2005, more than 81 percent of businesses with 50 or more employees had some form of health-promotion program, according to Wellness Councils of America, a nonprofit based in Omaha.
The organization also reported about 50 percent of corporate healthcare costs are lifestyle-related and, therefore, potentially preventable. With health insurance premiums rising 15 to 20 percent annually, many companies view spending a fraction of that on wellness programs as a reasonable investment.
Yoga is especially useful in terms of preventive care, said Dee Greenberg, owner of Om City Yoga in Cambridge, because it promotes harmony of the mind and body. "A lot of what people hear on the job is 'work harder, stay longer, be more productive.' Yoga is giving them an opportunity to de-stress," she said. "When they go back to their desks, their heart rate is changed, they're breathing different, and they're focused."
At Abt, McIntyre said, the firm has spent less than $5,000 each year since 2005 on the yoga program, as well as on workplace massages and Weight Watchers discounts. She said she hasn't evaluated what, if any, related savings there are on healthcare. Judging by input from employees, she said, it's working.
"If people are well, they're going to utilize their health insurance less. That means our claims are lower. Over time, it may even reduce our rates," she said.
At least in one secluded spot, the yoga benefit is already transforming the feel inside Abt.
On a recent Thursday in a basement room there, Dymek, the yoga instructor, shut off the overheard fluorescents, lined the room with Christmas lights, sprayed the air with a lavender mist, and put on a CD of New Age music.
At noon, workers streamed in and spread out their yoga mats in two neat rows. When everyone was quiet, Dymek opened the class: "Let us allow our ego to leave the room. Let go of our tension, our concerns and create a space where nothing else matters but listening to our own breath."
---------
THE BOSTON GLOBE, Op-Ed, MONIQUE DOYLE SPENCER
"The games drug companies play"
By Monique Doyle Spencer, January 29, 2008
IT'S BEEN 10 years since we started letting drug companies advertise their drugs on TV. Let's ban them again. You don't agree? Then you don't watch much football.
A football game is a three-hour nightmare. It is almost as bad as the drug marathons during Matlock reruns and Oprah. First, let's look at the football advertising "demographic," or what we call a "person," that advertisers are going after. They appear to be talking to a man. He is a guy with the trifecta of high blood pressure, high cholesterol, and hair loss.
They are trying to sell him insurance, because he has none, but he does have plenty of body odor. He drives trucks to the top of mesas, where he blares "This is Mah Countreeee" on his radio. He drinks heavily. To shave, he requires a system of blades designed by NASA. What kind of hair does this poor guy have, anyway? It can't be only on his face!
So? So now we tell him that some woman out there is so interested in him that he needs to buy a magic pill for you know what.
I've been watching too much football, I know. But I think they are prescribing the wrong medicine for this guy. He does not need to cure his ED. He needs medicines that don't exist: medicines that make you stop scratching yourself. Medicines that make you forget the adjusting your body craves. Medicines that make you stop thinking that ED medicine belongs on the television that you watch with your kids.
We also need medicines for football commentators that would help them to make any sense whatsoever. My long-suffering husband has begged me to stop repeating what they say because this ruins the game for him. Remember, I don't comment, I just repeat their words exactly: "Tom, they'd better score some points if they want to win this game!"
Of course, all advertising is deceptive, so maybe drug ads are no different.
After all, herds of beer drinkers rarely attract enthusiastic young women. Antidepressants don't actually make you want to take your dog for a really long run. Feminine products do not make you have intimate conversations with your mother. Deodorant is not really for odors caused by playing manly sports like football. Most body odor comes from sitting around watching TV in your own body fat and advertisers know it.
But once upon a time, only a decade ago, we could watch TV with our kids and not have to explain ED to them.
We filled their heads with violence, yes, and sugar cereals. Not satisfied, we had to add sex to the picture. Even the Powerpuff Girls have a character that is all vamp body with no face. A million kids a week tune in.
So maybe we have to start small, with just banning drug ads. We could have a 10-year rule about laws. Ten years is long enough to find out that a law was a really bad idea. Let's try 10 years off, then we can decide if we really want to bring them back.
Of course, by then maybe I'll be singing a different tune. I'm lucky to be so young that I'm married to a guy who earns his body odor honestly, drives a sedan, and is insured.
Men don't know that this trifecta is pretty much what we look for.
Well, that. And no hair.
-
Monique Doyle Spencer is author of "The Courage Muscle: A Chicken's Guide to Living With Breast Cancer."
---------
--

-
Emerson Hospital chief Christine Schuster (center) said former employees manipulated the hospital's earnings by misusing contractual allowances - the discounts hospitals give insurance companies on the "official" prices for services and procedures. (Joanne Rathe/Globe Staff/File 2005)
--
"Emerson Hospital misstated financials: Investigation finds senior executives created documents"
By Jeffrey Krasner, Boston Globe Staff, March 21, 2008
Two senior executives of Emerson Hospital in Concord created documents that misstated the hospital's financial condition over parts of its last three fiscal years, the hospital found after an investigation and audit that concluded last week.
The misstatements made the hospital's performance appear better than it actually was, at a time when it was seeking donations for a major expansion that is now nearing completion.
As a result, Emerson violated some promises it made to lenders. That, in turn, forced the hospital to reclassify some of its borrowing as short-term debt, a technical measure that could limit its borrowing ability.
Emerson has not missed any payments and officials said it is not in danger of defaulting on its bonds. The audit completes an inquiry that began last August when a midlevel manager noticed billing irregularities and told a supervisor, said chief executive Christine Schuster.
In all, the hospital had to wipe out $7.1 million in improperly recorded revenue. Because of accounting rules, however, it only had to formally restate its books for fiscal 2006.
The two senior executives - Dana P. Diggins, Emerson's chief financial officer, and Michael Collins, its controller - left Emerson last year. Officials declined to say whether they resigned or were fired. A third financial executive, who the hospital would not name, was let go.
The matter has been referred to the office of Attorney General Martha Coakley, said John M. Lowe III, chairman of the hospital's board of directors.
John O. Wilhelm Jr., interim chief financial officer, said the misstatements were accidental.
"They weren't aware they were misstating it - they thought they were correctly stating it, but they were wrong," said Wilhelm. "People make mistakes and they move on. That's life. They were big mistakes."
Diggins is now chief financial officer at Harrington Memorial Hospital in Southbridge. Collins is chief executive at Merrimack Valley Hospital in Haverhill. Neither responded to calls seeking comment.
Schuster said the former employees manipulated the hospital's earnings by misusing contractual allowances - a term that describes the discounts hospitals give to insurance companies on the "official" prices they charge for services and procedures. Each month, the hospital must adjust the amount of money it expects to receive to account for such discounts.
"The controller at the time overrode the estimates that the contractual allowance model was generating," said Schuster. "That resulted in an overstatement of revenue."
The restatement is particularly sensitive because the hospital is required to keep its lenders and bondholders informed of any changes in its financial condition. A failure to file audited statements can constitute a technical violation of the many promises and ongoing commitments lenders require of borrowers.
Footnotes to the restated financial results, by the accounting firm PricewaterhouseCoopers, state Emerson was "not in compliance with certain debt covenants" for a $3.9 million loan from Bank of America.
In addition, the footnotes state Emerson was not in compliance with covenants for a $63 million bond offering conducted in 2005 by the Massachusetts Health and Educational Facilities Authority, a quasi-public agency that facilitates borrowing for smaller institutions.
Wilhelm said that after the audit was completed, the hospital was able to forge a new agreement with Bank of America that waives the violations. He said that contrary to what PricewaterhouseCoopers reported, there was no violation of loan agreements with the Massachusetts authority.
"This was a fluid issue going back and forth with the auditors," said Wilhelm. "There were a lot of rewrites (to the footnote) and there was a little hurry-up at the end. We are not, and have not, been in violation of any of our bond covenants."
The facilities authority, which arranged the bond offering, declined to comment.
The restatement also comes at a difficult time for Emerson. The hospital made a small profit, $1.7 million, on its healthcare operations in fiscal year 2006. But in fiscal year 2007, it lost $8.1 million on healthcare operations. Some of the losses were offset by investment income, yielding a loss of $4.7 million for the most recent year.
For the first four months of the current fiscal year, the hospital has broken even. But officials said the results were dragged down by a series of one-time charges, some associated with the accounting problems.
In particular, the hospital paid $490,000 to FTI Consulting Inc. - a healthcare consulting firm hired to improve the hospital's financial operations - and about $100,000 to the law firm of Wilmer Cutler Pickering Hale and Dorr LLP, which conducted the investigation.
"The board was concerned when this came to light, but because Chris (Schuster) had kept us informed all along, we were comfortable we were taking the right steps," said Lowe, the chairman. "We're now focusing on regaining our financial strength."
-
Jeffrey Krasner can be reached at krasner@globe.com.
-
---------
Tuesday, May. 20, 2008
"The Value of a Human Life: $129,000"
By Kathleen Kingsbury, TIME Magazine
In theory, a year of human life is priceless. In reality, it's worth $50,000.
That's the international standard most private and government-run health insurance plans worldwide use to determine whether to cover a new medical procedure. More simply, insurance companies calculate that to make a treatment worth its cost, it must guarantee one year of "quality life" for $50,000 or less. New research, however, would argue that that figure is far too low.
Stanford economists have demonstrated that the average value of a year of quality human life is actually closer to about $129,000. To get to that number, Stefanos Zenios and his colleagues at Stanford Graduate School of Business used kidney dialysis as a benchmark. Every year dialysis saves the lives of hundreds of thousands of Americans who would otherwise die of renal failure while waiting for an organ transplant. It is also the one procedure that Medicare has covered unconditionally since 1972 despite rapid and sometimes expensive innovations in its administration. To tally the cost-effectiveness of such innovations Zenios and his colleagues ran a computer analysis of more than half a million patients who underwent dialysis, adding up costs and comparing that data to treatment outcomes. Considering both inflation and new technologies in dialysis, they arrived at $129,000 as a more appropriate threshold for deciding coverage. "That means that if Medicare paid an additional $129,000 to treat a group of patients, on average, group members would get one more quality-adjusted life year," Zenios says. Based on patient surveys, one "quality of life" year is defined as about two years of life on dialysis.
Zenios's conclusions arrive amidst mounting debate over whether Medicare, the U.S. government health plan for seniors, ought to use cost-effectiveness analysis in determining coverage of procedures. Nearly all other industrial nations — including Canada, Britain and the Netherlands — ration health care based on cost-effectiveness and the $50,000 threshold. Medicare, on the other hand, decides whether to pay for new technology based on whether a treatment is "medically necessary and appropriate." But as health care expenses rise and entitlement programs grow fiscally strapped — at least one part of Medicare is now expected to be bankrupt by 2019 — more and more academics have called for this approach to be reconsidered, and for cost to become a factor. Such a move would mean that "if the incremental cost of a new technology was more than the threshold," Zenios says, "then the recommendation would be that Medicare not cover that new technology."
Assigning a dollar figure to Medicare patients' lives may sound crass, but such valuations are routine in Americans' daily lives. Take, for example, the $500,000 death benefit the government pays families when a soldier is killed in Iraq or Afghanistan. Or the cost calculations that for-profit health insurers make to determine how much coverage they'll give customers. In fact, at least some Americans seem at ease with allowing money to play a prominent role in health care decisions. In a 2007 survey of New Yorkers, 75% of participants felt "somewhat" to "very" comfortable with allowing cost to inform Medicare treatment decisions, once they understood how the system worked. "Americans understand and are prepared to engage the issues that arise when setting priorities and limits for their public programs," Marthe Gold, the City University of New York Medical School professor who conducted the study, wrote with colleagues this past fall in the journal Health Affairs.
The Stanford researchers caution that if Medicare fully adopted a cost-benefit analysis model, too many patients could be denied life-saving treatment. They return to the example of dialysis patients. Their study showed that for the sickest patients, the average cost of an additional quality-of-life year was much higher — $488,000. "It is difficult to justify the burden and expense of dialysis when persons have other serious health conditions such as, for example, advanced dementia or cancer," says co-author Glenn Chertow, a nephrology professor at the Stanford School of Medicine. "In these settings, dialysis is unlikely to provide any meaningful benefit." But with organs including kidneys for transplant so scarce, is it justifiable to deny these patients a chance to live through dialysis? It is a question, Zenios says, everyone should approach with trepidation. "What is the true value of a human life? That's what we're asking people," he adds. "I wouldn't pretend to know."
---------
The Boston Globe, Op-Ed, ALISON BASS
"A dose of honesty in prescription drug ads"
By Alison Bass, June 2, 2008
LAST MONTH, a congressional committee held a hearing to examine the extent to which drug companies run misleading ads about their products. The committee spotlighted TV commercials for three drugs - the cholesterol-lowering drugs Lipitor and Vytorin, and the antianemia drug Procrit - and it raised concerns that the makers of these drugs had, in the words of Representative Bart Stupak of Michigan, aired "manipulative commercials designed to mislead and deceive" consumers.
Stupak, a Democrat who is chairman of the Energy and Commerce Subcommittee on Oversight and Investigations, called for new restrictions on direct-to-consumer ads and questioned whether pharmaceutical companies should be allowed to do such advertising at all. The United States is one of only two countries that permit those ads. Stupak's comments received little media coverage, possibly because Republican members of the panel kept questioning why the issue merited congressional attention.
Here's why it does. Little more than a year ago, my 83-year-old father was told he had a low red blood cell count, which could explain why he had been feeling tired lately. His doctor prescribed a high dosage of Procrit and my father started taking injections of the drug. He had no idea that high doses of Procrit and other erythropoiesis-stimulating agents can cause an increased risk of heart failure in patients with kidney problems, which he has had. Nor did he know that in March 2007, the Food and Drug Administration required black box warnings be added to the label of these drugs detailing the risks of taking them.
Five days after his first Procrit injection, my father had a mild heart attack - his chest felt constricted and he was having trouble breathing. My mother rushed him to the hospital, where doctors put two stents in one artery and used angioplasty to blow the other artery open. Yet even after his heart attack, my father continued to take Procrit at dosages higher than recommended by the FDA.
Why? Because that's what his doctor told him to do and he had seen and read nothing to caution him otherwise. To the contrary, print and television ads and labeling information for patients implied that Procrit could reduce fatigue and weakness in people with anemia.
Indeed, for seven years, Johnson & Johnson, which sold Procrit, aired TV commercials showing exhausted senior citizens suddenly revived after taking the drug. Similar claims were made on the labels for Procrit and another erythropoiesis-stimulating agent, Aranesp, even though both drugs were approved by the FDA only for their ability to reduce the need for blood transfusions.
While the Procrit TV ads were ostensibly targeted at cancer patients who develop severe anemia as the consequence of chemotherapy, the commercials seemed designed for a much broader audience.
As Dr. Otis Brawley, professor of hematology and oncology at the Winship Cancer Institute, told a FDA advisory panel meeting last year: "I think one of the most important issues here is that most doctors and most patients think that this drug has been approved because it improved quality of life. There is a lot of sleight of hand here with how this drug is used, what the drug is used for."
Johnson & Johnson took its Procrit commercials off the air in 2005, but did not change the erroneous labeling information until March 2007.
Until recently, Johnson & Johnson and Amgen, the maker of Aranesp and another erythropoiesis-stimulating agent, Epogen, also offered doctors millions of dollars in rebates for prescribing their drugs. Is it any surprise that all three became blockbuster drugs, with combined sales of nearly $14 billion in 2006?
At the congressional hearing in May, Stupak and Dingell pointed to the misleading Procrit ads as evidence of the need for more stringent oversight of drug advertising. But their message was repeatedly undercut by four Republican legislators, all of whom, it's worth noting, have received thousands of dollars in campaign contributions from drug companies, including the ones on the hot seat in May. At the hearing, the drug company representatives were quick to note that the ads under scrutiny - for Vytorin and Lipitor as well as Procrit - are no longer on the air.
That may be so, but Johnson & Johnson was just called to task for airing another TV commercial touting the benefits of a drug-coated stent that it makes. In an article in the New England Journal of Medicine, several cardiologists called the stent ads "potentially deceptive" because they focus "almost exclusively" on the device's benefits and neglect to spell out its risks. Sound familiar?
-
Alison Bass is author of "Side Effects: A Prosecutor, a Whistleblower, and A Bestselling Antidepressant on Trial."
-
---------
"Bureaucracy blocks health care reform"
By Peter Albertson, PITTSFIELD, Massachusetts
Tuesday, June 03, 2008
The best way to avoid the outrageous, ever-growing health care costs threatening many Americans with disaster is simply to die. That may sound drastic or cruel, but think about it. The insurance companies keep raising their rates and/or increasing their co-pays. Just don't get sick is their message, but many of them won't pay for preventive care. Of course, they don't want us to die because then they lose customers. Do I seem bitter? Yes, I am.
If you are really, really sick, make sure it's not an unusual kind of illness, just something ordinary like high blood pressure, or heart failure, or a kidney stone, or an infection. But, if you need one of the newly developed cancer or multiple sclerosis drugs, or any of the tremendously expensive drugs, your insurance company is going to make you pay a gigantic portion of the cost. If the disease doesn't kill you, your co-pay well might.
.
Here's a cute little story. This year my Social Security payment went up a bit — the usual cost-of-living increase. At the same time, my payment to the AARP-selected insurance company for prescription drug insurance, which is automatically deducted from my Social Security, also increased. So, I am now taking home less Social Security than I was last year. And what I must pay out of pocket for medicines has increased at the same time.
It's the insurance companies making the big bucks from the health-care industry. I believe most doctors want to care for their patients, help them, and make them and keep them well. But now, Medicare and the insurance companies are about to cut payments to doctors while reducing our benefits.
As The New York Times reported earlier this year, one woman, who had had the same insurance company for 17 years, went to the pharmacy to refill her prescription for Copaxone, a medicine for multiple sclerosis, which she has been taking for about eight years. It is an expensive drug, but it was covered by her insurance. She had a $20 co-pay for a month's supply of the medicine. But when she went to pick up her medication this time, the co-pay had zoomed to $325. Her annual cost would go from $240 to $3,900 and that would be for the rest of her life.
Here's another not so pretty tale from that Times article: A retired older man has to take Sprycel for his leukemia. This drug is supposed to block the growth of cancer cells and might extend his life, and he would not need chemotherapy infusions.
He has drug insurance through AARP; Sprycel, which he will have to take for the rest of his life, costs around $13,500 for a 90-day supply, and he discovered that his AARP insurance was now going to force him to pay at least $4,000.
In this country today there are something like 47 million people, almost 16 percent of the population, who have no medical insurance, thus no regular medical care. When they or their children get sick, they run to the emergency department (if there is one) of the local hospital (if there is one) to have whatever is wrong taken care of.
This of course can be a fearful experience, in itself. If you are sick, and you turn up at the ED and you need help, you sit and wait, and if it is busy night, you wait some more, and then some more. If you aren't dead by the time they call you in, you can get taken care of, maybe. That is a terribly inefficient and costly way to get your medical care if it is not a true emergency. It's another reason why the general level of health-care costs are increasing. (Let me mention that Pittsfield is special; I have never had to wait a very long time when I have turned up at BMC's emergency room and have always been very well taken care of.)
According to Physicians for a National Health Program (PNHP), and U.S. Centers for Disease Control and Prevention, "one-fifth of Americans can't afford one or more of the following services: medical care, prescription medicines, mental health care, dental care, or eyeglasses." The U.S. needs a health care program that will cover the uninsured and the underinsured, as well as the insured who pay the cost of insurance, watch it eat into their living standards and scare them about their retirement.
Clearly, we have to get the insurance companies out of the health care game. It won't be easy because they carry a lot of clout with Congress and they are big contributors to political candidates. Look at what's happened in Massachusetts: As pointed out recently by PNHP, the law here "imposes steep fines on the uninsured" if they don't buy the medical insurance they can't afford. And a whole lot of people have not bought in.
"Bureaucracy consumes 31 percent of U.S. health spending, versus 17 percent in Canada," wrote David U. Himmelstein, M.D., and Steffie Woolhandler, M.D., recently, in The Nation magazine. They went on to say: The "difference translated into $350 billion frittered away annually here, where a million health care workers, as well as hundreds of thousands in the insurance industry, spend their days on useless paperwork."
.
So, who's going to pay for improved medical care? The slogan that has been making the rounds seems a good one: "Medicare for All." First, understand that something like 60 percent or more of health care costs are now already paid by the federal government through our taxes. So, the money that goes into Medicare and Medicaid would go into a new national health program. Then we would have a small income tax, something between 2 and 4 percent; and a small tax on employer payrolls, about 7 percent. Those tax increases will probably be less than people now pay for insurance, medicines, and any other out-of-pocket medical-care expenses.
Except for that 7 percent payroll tax, employers would have no other expenses for health care. The income tax would take the place of all current insurance premiums, co-pays, deductibles, and other out-of-pocket payments. For most people, a 2 percent income tax would be less than they now pay for insurance premiums and out-of-pocket payments.
Even if this is not a perfect program and needs further tweaking, it's a helluva lot better than the chaotic, crazy, costly system we have now.
-
Peter Albertson is an occasional Eagle contributor.
-
---------
"Bush administration delays scheduled Medicaid cuts"
By Jim Abrams, Associated Press, July 1, 2008
WASHINGTON - The Bush administration said yesterday it is freezing a scheduled 10 percent fee cut for doctors who treat Medicare patients, giving Congress time to act to prevent the cuts when lawmakers return from a July 4 recess.
Physicians have been running ads hinting that as a result of the cuts, patients may find doctors less willing to treat them.
The administration's delay in implementing the cuts, which had been scheduled to go into effect today, spares lawmakers from having to use the recess to explain to seniors why they didn't do the job before leaving town.
Kevin Schweers, a spokesman for the Department of Health and Human Services, said yesterday the Centers for Medicare and Medicaid Services will hold doctors' Medicare claims for services delivered on or after July 1.
Claims for services received on before June 30 will be processed as usual, he said.
Congress, not willing to face millions of angry seniors at the polls in November, is expected to act quickly when it returns to Washington next week to prevent the cuts in payments for some 600,000 doctors who treat Medicare patients.
The cuts were scheduled because of a formula that requires fees to be reduced when spending exceeds established goals.
Health and Human Services Secretary Mike Leavitt had promised Friday that his agency "will take all steps available to the department under the law to minimize the impact on providers and beneficiaries."
Yesterday, the department used its administrative tools to delay implementing the 10.6 percent cuts.
"By holding claims for healthcare services that are delivered on or after July 1, [the Centers for Medicare and Medicaid Services] will not be making any payments on the 10.6 percent reduction until July 15 at the earliest," Schweers said.
Almost every year, Congress finds a way to block such cuts.
But last week the Senate fell just one vote short of the 60 needed to proceed to legislation that would have stopped the cut.
Doctors have complained for years that Medicare payments have failed to cover rising costs.
The bill is H.R. 6331.
---------
"Kennedy leads renewed effort on universal healthcare: Presses for bipartisan support before new president takes office"
By Lisa Wangsness, (Boston) Globe Staff, July 2, 2008
Senator Edward M. Kennedy's office has begun convening a series of meetings involving a wide array of healthcare specialists to begin laying the groundwork for a new attempt to provide universal healthcare, according to participants.
The discussions signal that Kennedy, who instructed aides to begin holding the meetings while he is in Massachusetts undergoing treatment for brain cancer, intends to work vigorously to build bipartisan support for a major healthcare initiative when he returns to Washington in the fall.
Those involved in the discussions said Kennedy believes it is extremely important to move as quickly as possible on overhauling the healthcare system after the next president takes office in January in order to capitalize on the momentum behind a new administration.
Kennedy was an early endorser of Senator Barack Obama, the presumptive Democratic presidential nominee who is also a member of the Committee on Health, Education, Labor and Pensions, which Kennedy chairs.
Obama's Senate staff has attended the roundtable discussions. If Obama is elected, Kennedy's effort to identify points of agreement among senators could smooth the way for the new administration to press ahead on universal healthcare, which Obama has promised to implement within four years.
The last time a national healthcare plan was attempted, under President Clinton in 1993, the presidential panel charged with devising a proposal was widely criticized for not consulting enough with Congress, and protracted disagreements erupted, delaying its progress for months and ultimately resulting in its demise. Kennedy's effort appears to be designed to identify areas of common ground between Democrats and Republicans, business and labor, providers and insurers, and others before the new president takes office.
"The senator is trying to learn from health reform attempts in the past and to build a fair amount of consensus among his Senate colleagues, House colleagues, and the Obama campaign . . . and find a strategy that could carry with some momentum into the new administration," said Dr. Jay Himmelstein, a health policy specialist at University of Massachusetts Medical School and a former Kennedy staff member who has been involved in the talks.
The initiative also suggests that Kennedy, who has made healthcare his signature issue in his 45-year Senate career and who is fighting an aggressive brain tumor, is considering his legacy as a new administration arrives in Washington - a moment many see as the best chance for widespread changes in the healthcare system in 15 years.
"You have got to think this will be the Ted Kennedy Health Reform Act, because he's a beloved figure and he's championed the issue for so long," said John Rother, policy director for the AARP, which has been involved in the discussions. "There are a lot of unknowns right now, but what we do know obviously is he is very close to Obama, and he also has quite a network of health policy experts that he can draw from."
Melissa Wagoner, spokeswoman for Kennedy, added that "Making sure each American has access to quality, affordable healthcare is the cause of Senator Kennedy's life."
Kennedy played a critical role in helping Massachusetts create a healthcare overhaul proposal in 2006 by aiding the state in obtaining the federal money needed to subsidize it. It appears he is now looking to Massachusetts to help shape the debate in Washington. Earlier this year, Kennedy recruited John McDonough, executive director of Health Care For All in Boston and a major player in the Massachusetts healthcare overhaul debate, to lead the new health initiative.
Aides to Kennedy have also assembled a network of Massachusetts advisers, including healthcare lawyers, economists, nonprofit leaders, doctors, and health insurers who may be asked to work on specific aspects of a national plan. At a recent meeting in Boston, the group discussed how different elements of the Massachusetts approach might work on a national level.
Rob Restuccia, executive director of the national healthcare advocacy group Community Catalyst and one of those who attended, said the group considered questions such as whether the Massachusetts Health Connector, the quasi-public entity that helps uninsured people obtain coverage, might be structured on a national level.
"I believe we will have a great story to tell about how national health reform can learn from what we've done in Massachusetts," said Jarrett Barrios, president of the Blue Cross Blue Shield of Massachusetts Foundation, who also attended one of the meetings.
Kennedy is not alone in trying to get a head start on the healthcare debate. Senator Max Baucus, a Democrat from Montana and chairman of the Senate Finance Committee, held a healthcare summit in mid-June, and a bipartisan proposal to make private insurance accessible to all Americans has been put forward by Senator Ron Wyden, a Democrat from Oregon, and Robert Bennett, a Republican from Utah.
Intraparty disputes were one reason Clinton's 1993 proposal foundered. Back then, Daniel Patrick Moynihan, the Democratic chairman of the Senate Finance Committee, dismissed the financing of Clinton's plan as "fantasy" just before the president presented it to Congress.
Ron Pollack, executive director of Families USA, a healthcare consumer advocacy group, said Kennedy was trying to avoid division by having senior staff members meet with their counterparts on Baucus's committee.
"If the two committees are working cooperatively together and developing a common legislative proposal, it means that the process is less likely to get bogged down because of jurisdictional and substantive differences," he said.
Even though health costs have soared along with the number of uninsured over the past 15 years, the defeat of the Clinton health overhaul plan was so politically devastating to the administration and to efforts to enact universal health insurance law that nothing approaching such a large-scale effort has been tried since. One purpose of the roundtable discussions, participants said, is to educate Senate staff on broad issues that have not been seriously debated in years.
Kennedy's committee has held two meetings so far - one with healthcare coalitions, the other with physicians' groups. Eight more will be held by the end of the month. The meetings are attended by aides for committee members of both parties, said Craig Orfield, a spokesman for Senator Mike Enzi of Wyoming, the ranking Republican on the committee.
Whether the two parties and myriad interest groups can overcome their differences over the next year remains to be seen, but several of those participating in the discussions expressed optimism about that possibility.
"There's been talk about the healthcare crisis for years, but I think in the last year and a half, the system is failing so many people and becoming so costly, that I don't think there's anybody who doesn't understand there's got to be fundamental changes to the system," Orfield said.
---------
"$40 Millioin Health Care Reform Campaign Launches"
July 08, 2008, 7:02 PM, ABCNews
ABC News' Molly Hunter Reports:
Health Care For America NOW, a new grassroots movement working to bring affordable healthcare to Americans, announced its launch at the National Press Club in Washington Tuesday.
The $40 million campaign will spend $1.5 million on their first round of national TV, print and online advertising and an additional $25 million in paid media over the next five months.
"We are here today to announce the beginning of a new movement in the United States," Campaign Director Richard Kirsch said in an announcement made simultaneously in 52 U.S. cities.
The first TV ad which airs on cable and illustrates the organization's strong opposition to the current health care system.
"We can't trust insurance companies to fix the healthcare mess," states the ad.
Health Care For America NOW is a coalition of over 100 organizations and unions. Many leaders of high profile organizations and unions including the American Federation of State, County and Municipal Employees, SEIU, AFL-CIO, United Food and Commercial Workers, Campaign for America's Future, Center for American Progress Action Fund, MoveOn.org and Planned Parenthood Federation of America were present in DC to speak at the launch.
Together with these organizations Health Care For America NOW "will mobilize millions of Americans to demand that the first order of business of the next President and Congress is to enact quality, affordable health care for all in 2009," Kirsch said. The campaign does not plan to endorse either presidential candidate or a specific health care plan.
Sen. John McCain's, R-Ariz., health care plan provides tax credits of $5,000 for families in order to buy health insurance, and Sen. Barack Obama's, D-Ill., plan mandates coverage for children and requires that employers share the cost of their employees' health coverage.
Kirsch challenges each American to make a choice.
"We will be asking Members of Congress this year to tell us if they are on our side or the side of the health insurance industry," he said.
Health Care for America NOW suggests three options to achieve universal health coverage. Individuals can stay with the private insurance they already have, join a new private insurance plan or choose a public health insurance plan.
"We are looking for a uniquely American solution," Kirsch said. "In our vision of healthcare reform, the government works for us."
The campaign aims to find a solution that is affordable for both people and businesses alike. USAction Executive Director, Jeff Blum, called the campaign, "the human rights movement of our time."
Leaders of the organizations echoed Kirsch and Blum's sentiments, calling for urgent and forceful healthcare reform.
Gerald McEntee, the International President of AFSCME, stated: "Today, we say enough is enough! No more needless delays. No more idle discussion. No more political posturing. We've talked long enough, we need action!"
Roger Hickey, co-Director of the Campaign for America's Future opted out of his prepared statement, instead saying, "Enough has been said, we are proud to be part of this coalition and we think we need to get on with the agenda. Let's move it!"
---------
"Kennedy, allies defend Medicare"
The Berkshire Eagle - Letters
Tuesday, July 15, 2008
Your editorial, "Kennedy to the rescue" (July 11) was aptly titled and appropriately described his efforts with regard to Medicare: champion. His courageous and inspiring appearance in Washington to vote for the Medicare Improvements for Patients and Providers Act, despite his own critical health problems, pushed the Senate to its veto-proof majority.
Not only does the bill preserve access to care for seniors and military personnel, but it's also a shot in the arm for physicians' medical practices, as it blocks a steep cut in Medicare physician fees and provides a small increase through 2009. Along with Senator Kerry's yes vote, Kennedy's action did "help keep Medicare strong." Let's remember, too, that every member of the Massachusetts congressional delegation voted for the bill when the House overwhelmingly approved it two weeks ago.
On behalf of physicians and patients throughout Berkshire County, to all our federal representatives, I say "Thank you."
DAVID GRYGIER, M.D.
Pittsfield, Massachusetts
The writer is president, Berkshire District Medical Society.
---------
The Boston Globe, Op-Ed, CHARLES KENNEY
"Finally, a little optimism on healthcare"
By Charles Kenney, July 30, 2008
SLOWLY BUT surely the long-held article of faith that the United States has the world's finest healthcare is eroding in the face of mounting evidence. A fresh report from the prestigious Commonwealth Fund concludes that "despite spending more on healthcare than any other industrialized nation, the US overall continues to fall far short on key indicators of health outcomes and quality."
The report found that even with lavish spending the United States ranked "last among 19 industrialized nations when it comes to premature deaths that could potentially have been prevented by timely access to effective healthcare."
Given the Commonwealth Fund reputation for gold-standard reports, this work is taken seriously throughout the healthcare world. And while it is discouraging in many ways, there are elements within the study that are cause for optimism.
Dig deeper into the report - and look around at other indicators, as well - and it becomes clear that there are important trends in healthcare today which bode well for a future of improved quality. While incremental steps do not guarantee system transformation, these trends signal a dramatic new direction - perhaps one that will lead to a transformed healthcare system:
Institute for Healthcare Improvement campaigns. More than 3,700 hospitals throughout the country have enlisted in a coordinated attempt to protect millions of patients from preventable errors such as medication mistakes, surgical complications, pressure ulcers, and much more. Karen Davis, president of the Commonwealth Fund, wrote that her recent study shows that "performance on a key measure of patient safety - hospital standardized mortality ratios, which were targeted in the Institute for Healthcare Improvement's [campaigns] - improved significantly, by 19 percent from 2000-2002 to 2004-2006."
Measurement of clinical quality. The trend toward measurement of clinical outcomes is irreversible. Regulatory agencies as well as businesses and consumer groups now insist on data measuring the quality of care in a wide variety of clinical areas. Individuals want to know which cancer surgeon has the best record, companies want to know which physician practice provides the best quality care for chronic diseases, and everybody wants to know which are the safest hospitals. (Transparency - opening up critical data for the world to see - goes hand-in-hand with measurement.)
Adoption of electronic health records. Increasingly, large physician practices and hospitals have upgraded from paper files to electronic health records. The best systems not only provide clinicians with all relevant information about a patient, they also offer clinical guidance that improves safety (averting medication errors, for example) and quality. A New York Times story in June indicated that a New England Journal of Medicine survey found that "82 percent of those using such electronic records said they improved the quality of clinical decisions, 86 percent said they helped in avoiding medication errors, and 85 percent said they improved the delivery of preventative care."
Improved quality for some chronic diseases. Billions of dollars are spent each year on patients with chronic diseases who do not receive the recommended care designed to keep their conditions under control. Yet the Commonwealth Fund study reports a significant improvement in control of diabetes and high blood pressure - an extremely encouraging development.
Growing awareness that quality equals affordability. This may be the most encouraging trend of all - the increasing awareness that the way to control costs is to provide higher quality care. The belief is that quality care for chronically ill patients, for example, keeps them healthier and out of the hospital, saving enormous amounts of money. Thus the trend toward creating contracts that call for providers to be paid not on the basis of procedures but on the basis of outcomes. Under this approach doctors who provided all the care needed to a population of diabetics, for example, would be improving their patients' lives and rewarded financially.
Transforming the US healthcare system so it provides safe, high-quality care at a reasonable cost will not be easy. Not only is it not a sprint, it is a marathon - uphill and in the rain. But these and other indications hold out the promise that plugging away, we just might get there.
-
Charles Kenney's new book, "The Best Practice: How the New Quality Movement Is Transforming Medicine," has just been published.
-
---------
The Boston Globe, Op-Ed, ROBERT POZEN AND CATHY SCHOEN
"How rehospitalizations are hurting Medicare"
By Robert Pozen and Cathy Schoen, August 14, 2008
GETTING Medicare costs under control is no easy job. Congress recently overrode a scheduled 11 percent cut in Medicare's physician fees by freezing them for the rest of 2008 with a slight raise in 2009. But the program's finances will continue to worsen as baby boomers retire. Avoiding deep cuts in physician fees from 2010 onward will require a $20 billion fix every year for the following decade.
But there is a straightforward way to pay for half of this fix. Medicare spends vast sums on hospital care for patients readmitted within 30 days of their previous stay in a hospital. These readmissions are often avoidable. And if Congress focuses on reducing the need for rehospitalization in areas where the practice is most common, Medicare could save many billions of dollars.
The percentage of Medicare patients readmitted to the hospital within 30 days averaged 18 percent in 2005 - based on an analysis by the Commonwealth Fund of 30 prevalent medical conditions. But the readmission rate varies from area to area. Near the low end, 12 percent of hospitalized patients were readmitted in San Jose and St. Paul; near the high end, the rate was 22 percent for Las Vegas and St Louis. Boston's rehospitalization rate, 19 percent, was 1 percentage point greater than the national average.
According to a Medicare Payment Advisory Commission study, 75 percent of all 30-day hospital readmissions in Medicare in 2005 were potentially preventable - or 13 percent of total admissions. This represents a potential savings to Medicare of $12 billion in one year. To realize these savings, Congress should focus on three objectives: decreasing complications during hospital stays, improving patient communications in the discharge process, and monitoring patients after discharge.
Higher rates of hospital readmissions are associated with infections and other complications acquired by patients during hospital stays. Under traditional procedures, Medicare can pay a higher rate for hospital stays involving complications, or can pay for readmissions due to complications or medical errors. In a pilot project in which hospitals were paid bonuses and held accountable for better outcomes, quality improved and readmission rates fell substantially.
Another main cause of preventable readmissions is poor communication with patients in the discharge process, especially regarding medications. One hospital cut readmission rates by giving cardiovascular patients a checklist of indications for five medications to prevent complications. Some hospitals have had success providing patients at discharge with a "transition coach" to review their medication needs, supply a copy of their health records, and encourage timely follow-ups.
The most important cause of rehospitalization is insufficient monitoring of patients after discharge. For example, Hackensack University Medical Center asked nurses to telephone cardiac patients after discharge to check on health indicators like weight, swelling, and shortness of breath. These calls led to a 78 percent drop in the center's readmission rate for such patients. Similarly, studies have found that properly timed follow-up visits to doctors will reduce rehospitalization rates. These studies suggest that the optimal time for such visits is 5 to 10 days after discharge. However, another study found that at most one-third of physicians received complete discharge summaries at the first post-discharge visit.
Unfortunately, Medicare does not pay hospitals for most mentoring or monitoring procedures during or after patient discharge. Medicare should bundle extra payments for these procedures as part of the initial hospital stay - and claw back the additional payment for any patient who is readmitted to any hospital within 30 days.
Medicare needs to create the right incentives. Now, if a hospital succeeds in reducing readmissions, it will lose revenues because Medicare will be paying for fewer second stays. By contrast, if a hospital increases its readmission rate, it will receive more revenues because Medicare will pay for both hospital stays.
Congress should require hospitals to publicly disclose their readmission rates. Furthermore, any hospital above the national average for readmissions should receive a lower rate from Medicare for the second hospital stay. Any hospital with a lower readmission rate than the national average should receive a bonus payment from Medicare for the first hospital stay.
With the right incentives in place, Medicare should generate over $100 billion in savings over the next decade by bringing the high-cost areas down to the national average on 30-day rehospitalizations.
-
Robert Pozen is a trustee of the Commonwealth Fund. Cathy Schoen is senior vice president of the Commonwealth Fund.
-
---------
"Sex, Massages and Taxpayer Dollars: Researchers Look at Random Sex, Beauty, and the Obvious"
By SCOTT MAYEROWITZ, ABC NEWS Business Unit, Aug. 20, 2008 —
If you had $147,000 to spend on scientific research, would you rather try to find a cure for cancer or see whether women get sexually aroused while watching pornography?
Or how about this: How much would you spend to learn whether men or women are more likely to sleep with a stranger?
Or maybe you want to learn whether athlete's muscles feel more relaxed after getting a massage. Seems kind of obvious, right?
Each of those questions has been studied by academics, and in most cases taxpayers have foot the bill, sometimes to the tune of tens of thousands of dollars.
"Oftentimes academic researchers will get government grants to do things that you've got to wonder: Why are they doing that?" said Merrill Goozner, director of the integrity in science project at the Center for Science in the Public Interest. "There's plenty of research out there that doesn't need to be done, and why somebody funds it is one of the great mysteries of life."
Porn Sexually Arouses Women
The National Institutes of Health has an annual budget of $29.5 billion. The overwhelming majority of that money goes out in grants to researchers around the country and funds the agency's internal research.
The average amount awarded in research grants last year was $403,528. Most grants tend to cover broad research topics, making it difficult to zero in on the cost of a specific paper or study.
Still, these studies occasionally raise a few politicians' eyebrows.
A few years ago, NIH gave a $147,000 grant to a Northwestern University psychology professor who was paying women to view pornography while a device measured their sexual responses.
That study didn't go over too well in the halls of Congress.
Arizona Rep. Jeff Flake was among 20 Republicans to sign a letter to NIH's director asking for an explanation for why taxpayer money was going for such a study. They called it "a bizarre spending decision."
Today, Flake believes Congress has failed to properly oversee NIH and its spending.
"It's Congress' job to set guidelines for how NIH and other agencies spend taxpayer money and then exercise oversight to ensure that those guidelines are being followed. "However, over the last several years, Congress has neglected its oversight function," Flake's office told ABC News. "It's difficult for Congress to criticize NIH for wasteful grants when Congress itself is earmarking billions of dollars every year on similarly wasteful pet projects."
A spokesman for NIH declined to comment about studies that some consider a waste of tax dollars.
While discovering whether porn arouses women may not seem to warrant a hefty price tag, Goozner points out that you never know when something seemingly silly could lead to the next miracle discovery. "Certainly, some of these questions are more significant than they are made to appear when they're poked fun at," he said. Any outrage over government-funded research, from both Congress and watchdogs, tends to focus on industry-financed research, he said. "Industry funds a lot of research that often helps its bottom line. That shouldn't surprise anyone," Goozner said.
Sen. Charles E. Grassley, R-Iowa, has criticized NIH and the way the agency handles its grants. Grassley recently said the agency failed to oversee conflicts of interest in its grants. Many of those grant recipients also get money from drug companies. Grassley has accused NIH of not doing a proper job of requiring all of its grant recipients to also disclose their other funding sources.
Grassley's office declined comment for this story, but in a letter to the Senate Appropriations Committee, the senator wrote, "Researchers need to be put on notice that government grants come with obligations of financial disclosure."
Tax Research? Publish or Peril
Marc Abrahams, editor of Improbable Research, an organization that tracks unusual research studies, said that with roughly 100,000 medical journals published in the United States, part of the reason there are so many studies is simply because of the way academia works.
"In order to get hired, in order to keep your job and to get promoted, you have to publish a lot of studies," Abrahams said. "There are an awful lot of studies that were done apparently because somebody needed to get some more things on their resume."
NIH recently funded a study that proudly proclaimed the benefits of a massage to athletes after exercise.
Yes, that's right, your tax dollars helped conclude that a Swedish massage -- combining long strokes, kneading and friction techniques on muscles and various movements of joints -- can make you feel better after working out.
Granted, the researchers didn't use humans for this study. Instead they used sedated rabbits. The grant is part of a larger research program at Ohio State University and officials there said they can't break out how much money from NIH went to this specific research.
Random Sex: Men More Likely
Also in the category of things scientists have spent money to determine: Men are much more likely than women to have random sexual encounters.
In a 1989 study by two state college professors, titled Gender Differences in Receptivity to Sexual Offers and published in the Journal of Psychology and Human Sexuality, men and women were asked to randomly approach strangers of the opposite sex on a college campus and say: "I have been noticing you around campus. I find you to be very attractive," and then invite the strangers to have sex.
Guess what? "The great majority of men were willing to have a sexual liaison with the women who approached them," the study determined. "Not one woman agreed to a sexual liaison."
Abrahams said there's some questions that people really want answered, but there "are also a lot of studies that, to me, don't seem to be done for any reason."
Referencing the random sex study, he said, "It's still hard to figure out: What did they hope to learn by this?"
But he also cautioned that just because a study seems frivolous doesn't mean that it doesn't have any merit -- it might just be hard to understand the value now. Scientists who worked on electricity, the telephone or the Internet planned and studied for years before the fruits of their labor were realized.
The rules of science dictate that even the most common sense understanding must be proved, including things that sound logical or appear to be common sense.
"People study things because they are trying to understand things they don't," Abrahams said. "There are often a lot of problems that seem trivial, unless you happen to encounter it. If you or a relative get that disease, then it becomes the most important thing in the world."
Beer Goggles Really Exist
And don't think that this is just a U.S. epidemic.
Across the pond in Great Britain -- home to roughly 58,000 pubs -- a researcher just published a study that determined that, when drunk, women find men more attractive.
Marcus Munafo, a researcher in experimental psychology at the University of Bristol in England, funded his study through a $60,000 grant from the Alcohol Education and Research and Council, a group founded by the British Parliament.
Munafo concluded that with just a little bit of alcohol consumed in a short period of time, people find others roughly 10 percent more attractive than when they are sober.
The results of the study indicate that as little as a large glass of wine or a pint-and-a-half of beer is enough to make the girl or guy sitting on the bar stool next to you appear more attractive than you might otherwise think.
Munafo said the research is part of a wider program of studies looking at how alcohol modifies face perception and "cost almost nothing." He said his research is really focused on the behaviors that are more common after drinking, such as unsafe sex or violence.
"Our hypothesis," he said, "is that this might in part be because we begin to process emotional cues in faces differently after we've consumed alcohol."
---------
"Number of uninsured drops; poverty holds steady"
By Ricardo Alonso-Zaldivar, Associated Press Writer, August 26, 2008
WASHINGTON --The number of people without health insurance fell by more than 1 million in 2007, the first annual decline since the Bush administration took office, the Census Bureau reported Tuesday. Incomes edged up for the middle class while poverty held steady.
The numbers represent a scorecard on President Bush's stewardship of the economy at the kitchen-table level. But they only went as far as the end of last year, before the current economic downturn started gathering force. Although there were some bright spots, it was a mixed picture.
While the overall poverty rate held steady at 12.5 percent, poverty did rise among some groups. Latinos, children and the foreign-born -- demographic categories that overlap considerably -- experienced significant increases.
And while the number of uninsured dropped to 45.7 million, down from 47 million in 2006, it was largely because more people were covered through government programs.
For the middle class, the median -- or midpoint -- household income rose to $50,233, a modest increase of $665 from the previous year, although it was the third consecutive annual rise.
"The gains that occurred last year were welcome, but unfortunately, they are too little, too late," said Jared Bernstein, a senior economist with the liberal Economic Policy Institute in Washington. "The median household is no better off now than they were back in 2000, despite their deep contribution to the nation's economic growth during this period."
For example, after adjusting for inflation, last year's median household income of $50,233 was not significantly different from the figure for 2000, which was $50,557. "The American work force is baking a bigger economic pie, but the slices haven't grown at all," Bernstein said.
But White House spokesman Tony Fratto said the household income and health insurance numbers are definitely good news.
"It's clear that the long period of strong economic growth we were in had a positive impact for most Americans," Fratto said. "Obviously today we're dealing with higher energy prices and the downturn in housing, but the economy is showing enough resilience to keep growing in spite of those challenges."
Republican candidate John McCain distanced himself from the White House response, saying in a statement, "Too many of our neighbors are living in poverty, too many can't find a job, and too many are living without health insurance." The Arizona senator pledged tax cuts and policy changes to make health care more affordable.
Some analysts said that global trends, not just administration policies, are shaping the economic fortunes of individual Americans.
"Presidents like to take credit when things go well, and therefore they should get the blame when things don't go well, but there are lots of things driving this, not all of which are home grown," said Douglas Besharov, an expert on poverty at the business-oriented American Enterprise Institute. "The oil shocks are not. And globalization, which on balance is good for the country, leaves winners and losers."
The Census report was immediately swept up into presidential politics. Democratic presidential candidate Barack Obama's campaign fired off a statement blasting what it called the "failed record" of Bush's economic policies and promising "bottom up economic growth" if the Illinois senator is elected.
Overall, the Census found 37.3 million people living in poverty in 2007, of which 13.3 million were children. The poverty level for a four-person family in 2007 was $21,203. Among age groups, seniors had the lowest poverty rate at 9.7 percent, while children had the highest at 18 percent. The poverty rate for 2006 was 12.3 percent, but the change in 2007 was not statistically significant.
The welcome news on health insurance coverage was tempered by the continued erosion of private coverage paid for by employers and individuals. Government programs -- such as Medicaid for the poor -- picked up the slack, resulting in the overall reduction in people without health insurance.
The uninsured rate also fell to 15.3 percent, down from 15.8 percent in 2006.
"Private insurance has been falling (and) public insurance definitely went up," said David Johnson, who oversees the Census division that produced the statistics. The number of uninsured children also fell in 2007, after an increase in 2006 that had interrupted years of progress in getting more kids covered.
But seen over a longer period of time, the health insurance numbers are not reassuring. The number of uninsured -- and the rate -- are higher today than they were at the outset of the Bush administration in 2001. That year, 39.8 million people, or 14.1 percent, were uninsured.
"The number of uninsured is considerably higher than when the president took office, and in each year since then, employer-sponsored insurance has continued to diminish," said Ron Pollack, executive director of Families USA, a liberal group advocating coverage for all.
Stuart Butler, a top health policy expert at the conservative Heritage Foundation, said employers are scaling back on providing health care coverage because costs keep rising.
"I think it's more like we are seeing a tide that I don't think anybody can easily fix, particularly in the small-business sector," said Butler.
The Census report also underscored the growing role of women in the workplace, finding the gap between the earnings of women and men has shrunk to an all-time low.
In 2007, women working full-time, year-round averaged 78 percent of what men earned. But the gender gap varied considerably depending on the industries and types of jobs involved. And the good news for women may not necessarily be a positive for family incomes. The Census found that a major reason the gap is shrinking is that men's earnings have been fairly flat.
-
On the Net:
Census report: www.census.gov
---------
"Medicare faulted on audits for fraud: Big losses cited on medical gear"
By Christopher Lee, Washington Post, August 26, 2008
WASHINGTON - The rate of improper payments, including fraud, in Medicare's purchases of wheelchairs and other home medical equipment is significantly higher than the government has estimated, according to a federal audit released yesterday.
The report by Inspector General Daniel Levinson at the Department of Health and Human Services found an "error rate" of almost 29 percent in a sample of claims paid in 2006 under Medicare's multibillion-dollar durable medical equipment program. The Centers for Medicare and Medicaid Services had estimated a rate of 7.5 percent, or about $700 million in improper payments.
Investigators reviewed a sample of 363 claims to determine whether the Medicare contractor that routinely checks such claims had found all of the improper payments. Such payments include not only fraudulent claims, but also those without sufficient documentation and those for goods deemed not medically necessary. The new review found 20 payment errors that the contractor identified and 73 that it had not.
"We attributed these review discrepancies to the . . . contractor's reliance on clinical inference rather than additional medical records available from health care providers, CMS's inconsistent policies regarding proof-of-delivery documentation, physicians' lack of understanding of documentation requirements and CMS's lack of procedures for obtaining information on high risk [durable medical equipment] items from beneficiaries," Levinson wrote in a cover letter for the report.
Levinson recommended that Medicare auditors check a broader range of records underlying the claims, including physicians' records and other medical documents showing the necessity of the equipment. He also recommended the contractor be required to contact beneficiaries who allegedly got power scooters and other devices, which are considered at high risk for improper payments, to confirm that they were received and to determine whether they were medically necessary.
Timothy Hill, chief financial officer for the Centers for Medicare and Medicaid Services, said reviewing claims is one way the agency detects fraud. He said the agency implemented changes last year to help reduce the error rate, including a requirement of more documentation from doctors who prescribe wheelchairs for patients.
The inspector general's report "did point out some gaps in the program, some of which had already been addressed," Hill said.
Hundreds of millions of dollars are at stake in reducing payment errors. The durable medical equipment program, which costs more than $8 billion annually and pays for power wheelchairs, hospital beds, oxygen supplies, and other equipment for home use, has long been considered vulnerable to waste, fraud, and abuse.
A July report by the Government Accountability Office, for instance, found that Medicare has paid as much as $92 million since 2000 to suppliers who billed the government for equipment purportedly prescribed by doctors who were dead at the time.
---------
"Medicaid is now the biggest target on the scene"
August 25, 2008 at 11:30 am by Alan Chartock
Source: blogs.timesunion.com/wamc/?p=285
Now that Governor David Paterson has embarked on a series of cuts designed to rescue New York from a crippling fiscal deficit, a single program keeps rearing its ugly head. That program, Medicaid, has long been one of the most controversial of New York’s security blanket programs for those with the least resources. Medicaid is a bit of an enigma. As every politician seems to tell us on a fairly regular basis, New York’s Medicaid system is the “Cadillac” of all state Medicaid programs. It appears that New York Medicaid spends more money than California and Texas combined. That’s amazing. But even more amazing is the fact that many doctors in New York will not participate in the program because the fees they get are not even close to what they get from other insurers. How can that be? Several knowledgeable people have told me that Medicaid in New York helps our hospitals and nursing homes to the extent that many of them could not stay alive otherwise.
Of course, there is one other thing that infuriates New Yorkers and costs them money — the program seems to have its share of fraudsters, people who see it as a tree on which green money grows, there for the picking. Former Governor Eliot Spitzer was fully aware of the substantial Medicaid fraud perpetrated by some doctors and providers. He reached out to his network of attorneys and prosecutors and chose a brilliant criminal prosecutor from the U.S. Justice Department to become the New York State Medicaid Inspector General. His name is James Sheehan and he takes no prisoners. He is working hand in hand with both Attorney General Andrew Cuomo (who has the responsibility for prosecuting these cases) and criminal justice agencies on every level including the FBI, state and local police forces.
There are numerous ways in which he catches the crooks but one way is the technique now known as data mining. New York has developed a very sophisticated program that is able to look at all the mandatory reporting data, including what doctors and nursing homes charge. Some of the folks see a patient or client just one time but continue to send in bills for subsequent visits that never happened. Of course, some of the providers claim that it was administrative or clerical error, but sometimes it is purposeful and these folks get prosecuted and some actually end up in the hoosegow. I know one doctor who had to do his time on weekends while he was allowed to work all week. That was years ago and it is my impression that the criminal justice agencies are now out to make examples of people who try to bleed the system.
New York’s Medicaid system is breaking the backs of the counties which are charged with administering the program within their jurisdictions. The federal government pays a third, the state pays a third and, up until a few years ago, the counties paid a third. This so threatened the counties and their tax payers that there was massive push back from the county politicians. The state legislature and the governor agreed to put a cap on how much the counties would have to contribute, with the state “eating” the overage.
Needless to say, the state’s hospitals are quite worried right now. With the so called “tax cap” revolution in full swing, the counties are looking for more relief and the very expensive Medicaid program is at the top of everybody’s list for changes. There are many who want the state to take over the counties’ shares. In the rather unlikely event that happens, you can look for cuts in the program and that’s where the state’s very powerful health care unions get involved. These unions can make or break a politician. They have been known to mount massive media campaigns portraying politicians as out to hurt the poor and middle class and to endanger hospital health. In the past, they have won. One pathetic casualty was former governor George Pataki who has been accused of selling his political soul to former union health care czar, Dennis Rivera.
Fiscal crises like the one that we’re in currently have one good feature: they offer politicians the opportunity to stand up and say, “This has got to be done now.” At this juncture, the tax payers may well be in a mood to listen since their tax bills have become so onerous. Just remember that Medicaid is now the biggest target on the scene.
--
Posted in Alan Chartock
--
2 Comments -
Before I had my son (15 months ago), I worked as a therapist in the addictions and mental health (umbrella behavioral health) fields. I was at clinics managed by hospitals in the region. The majority of the clients seen in these clinics had Medicaid or Medicaid Managed Care (i.e. Medicaid and CDPHP, for example). The history with Medicaid is that it was basically understood that there was no cap on visits for these clients. They could just keep coming for years and no one would say anything. For clients with private insurance (for example Blue Cross), there would be a review with the clinician and the insurance representative every, say 10 visits, to justify continued visits. Furthermore, most private insurance gives 30 outpatient visits per year, and when it’s up it’s up. With private insurance, the practitioner had to develop the treatment plan around the number of visits a client had and also take into account the time of year the treatment is taking place. For example, if the client comes in in January, you don’t want to use up all the visits by March and then they have no outpatient visits left for the rest of the year in case they relapse. The problem comes in that people on Medicaid had often progressed in their disease more so than those with private insurance (they were on SSI/SSDI and not working to qualify for private insurance), so they did need more treatment or more intensive treatment in many cases, but it was also kind of like no accountability like with the private insurances. I don’t think it’s unreasonable for Medicaid to tighten up and start operating more like the private insurances do, at least in making therapists more accountable for a usable treatment plan with a realistic timetable.
Comment by MandyB — August 25, 2008 @ 6:22 pm
It’s quite obvious that the medicaid system is “broke.” There are not enough taxpayers to support this program which is out of control.
Comment by Rebecca — August 26, 2008 @ 5:44 am
---------
-
www.boston.com/bostonglobe/editorial_opinion/oped/articles/2008/09/13/a_doctor_and_patient_partnership/
-
---------
-

-
Boston Globe - health columns - Judith Ursitti, with daughter Amy, 8, and son Jack, 5, said that ''autism crosses a line from an educational issue to a medical one.'' (Mark Wilson/Boston Globe Staff)
-
"Push on for insurers to share autism costs"
By Erica Noonan, (Boston) Globe Staff, September 16, 2008
DOVER - Because of his severe autism, the cost of educating 5-year-old Jack Ursitti runs $100,000 a year. But unlike expenses with most medical conditions, the bills for treating him will be borne by Dover schools and the rural town's taxpayers - not his family's medical insurance.
Now, the nation's largest autism advocacy group, Autism Speaks, is planning a legislative push in 20 states, including Massachusetts, to require private insurance companies to pay a portion of the intensive, expensive educational treatments that many medical professionals say are a child's best chance to overcome, or just learn to cope with, profound and lifelong developmental and learning disabilities.
Similar laws have passed in the past several months in Arizona, Florida, Louisiana, and Pennsylvania requiring private insurers to pay toward a variety of therapies, including applied behavior analysis. That system, known as ABA, involves a weekly regimen of more than 30 hours of intense, often one-on-one, positive reinforcement techniques for teaching children how to speak, play, learn, and function in the world.
But private insurers are balking at the proposed requirement, especially coverage of the specialty ABA programs, which they say are relatively new and unproven, and not effective for all children. ABA teachers are not licensed in many states, and insurers contend that the therapy system is still too new to be regulated sufficiently.
Requiring insurers to pay for educating autistic children would "drive up costs for everyone," said Dr. Marylou Buyse, president of the Massachusetts Association of Health Plans, an industry group representing 12 health plans operating in the Commonwealth.
Health insurers should not be dragged into the educational arena, particularly to pay for ABA classes, she added. "In a sense, it's asking for a blank check for therapies that we'd want more evidence to prove are really effective," Buyse said.
But parents of autistic children are determined to get their youngsters into programs that offer even a glimmer of hope. They also want to shift society's perceptions of autism.
"If my son couldn't hear and needed a cochlear implant, we wouldn't be asking the school system to take responsibility," said Jack's mother, Judith, coordinator of the New England lobbying effort for Autism Speaks. "As a society, we have to acknowledge that autism crosses a line from an educational issue to a medical one. Jack was diagnosed by a neurologist, not a schoolteacher."
Richard DeRoo of Reading, a software engineer whose 11-year-old son, Evan, has autism, said parents are desperate for more financial help.
Since his diagnosis at age 3, Evan has needed extensive behavior, speech, physical, and occupational therapy, his father said. The family paid for some of that care out-of pocket at a cost of $25 to $50 per hour.
Evan is now at the Melmark School in Andover, a program that is paid for by the Reading schools systems.
"As a parent you wonder what more he's capable of, and I think he's capable of even doing so much more," his father said. "But people like us do not have the means to pay for this."
In 2007, the state reported that the number of schoolchildren diagnosed with autism had nearly doubled in five years, to more than 7,500. An estimated 1 in 150 children fall somewhere on the autism spectrum.
Educators have traditionally treated autism like other serious disabilities such as Down syndrome and cerebral palsy, which entitle a child to state-funded, Early Intervention weekly therapy sessions until age 3. Then the local school system takes over, paying for a spot - and sometimes an aide - in a public classroom, or, if the child's needs are more profound, a slot in a private school until adulthood.
Autism Speaks says there isn't enough money in school budgets to provide the therapy needed by the swelling numbers of autistic children, and it will be years before enough ABA-trained therapists can be hired into most public school classrooms.
"Autism is a complex disorder and it's taken folks a while to learn what we need to do," said Elizabeth Emken, the group's vice president of government relations. "But now we are talking about medical treatments prescribed by medical doctors, and covering them like any other medical treatments."
In Massachusetts, school systems already spend more than $1.6 billion annually on all special education programs. Some school districts currently spend more than 20 percent of their budgets exclusively on special ed students with a variety of needs, said Paul Andrews, director of government services for the Massachusetts Association of School Superintendents.
"Special-needs costs have escalated so high that it has reduced the amount of funding we can spend on regular education," said Andrews, a former school superintendent in Woburn.
The attempt to persuade state lawmakers to require autism coverage in Massachusetts is just getting off the ground, and Autism Speaks will soon be seeking a legislative sponsor and the support of local autism advocacy groups, Emken said.
The group will also focus political efforts in New York, New Jersey, Virginia, and Ohio over the next six months, and renew efforts in Oklahoma, where the mandate passed in the state Senate, but was killed in the House of Representatives this year.
Efforts to pass autism coverage requirements have not succeeded over the years on Beacon Hill, where bills failed to gain much momentum or widespread public support.
This latest attempt may turn out to be different, as the needs of autistic children and the financial stress on school systems have become too intense to ignore, said Vincent Strully, founder and CEO of the Southborough-based New England Center for Children, a program treating 400 autistic children at campuses in the Boston area and overseas in Abu Dhabi, United Arab Emirates.
"We have an enormous problem and no financial support to treat it. And we are in a race with the clock. We know that with two to three years of effective interventions in very young children, between 10 and 40 percent of them may even lose their diagnoses," Strully said.
The Massachusetts Association of Health Plans has not calculated what such a requirement could cost ratepayers, but insurers in other states put the price tag in the tens of millions, depending on the programs. Autism Speaks disputes those figures and says its proposal will increase health insurance premiums an average of 1 percent nationwide.
The health plan group said the state's new mental health parity law - which requires insurers to cover mental health treatment for people with substance abuse, eating disorders, and autism - offers families relief.
Longtime special education advocates raise another worry: If a private insurer is available to pay the tab for certain therapies, strapped suburban school systems may stop investing in their own programs.
-
Erica Noonan can be reached at enoonan@globe.com.
-
---------
DUELING HEALTHCARE PROPOSALS
The Boston Globe, Letters
"Do away with work-based insurance"
September 28, 2008
THE SEPT. 21 editorial criticizing John McCain's healthcare plan for moving the country away from work-based insurance is misplaced. There is little logic to basing the cost of medical insurance premiums on employment status. Workplace insurance arose during World War II because wage controls allowed employers to compete for workers on the basis of benefits only.
Basing premiums on group affiliation makes sense only when there is a statistical relation between the composition of the group and the financial risk to the insurer. For example, older people pay more for life insurance because their heirs are more likely to make a claim in the coming year, and novice drivers pay more for auto insurance because they have more accidents. Unless you work in a hazardous environment, the number or average age of your co-workers has little bearing on your likely healthcare requirements.
Administrative cost advantages associated with group affiliation could be achieved by establishing healthcare purchasing groups independent of employment, benefiting the unemployed and self-employed as well as the company employee. The time for work-based insurance has long since come and gone.
WILLIAM H. LEVISON
Lexington, Massachusetts
---------
The Boston Globe, Op-Ed, By Michael Hochman & Danny McCormick, October 1, 2008
MICHAEL HOCHMAN & DANNY MCCORMICK: "The media's role in healthcare"
WHILE THE pharmaceutical industry plays a vital role in the healthcare system, company profit motives can corrupt medical decision-making. In particular, company-funded research may be biased in favor of products made by the sponsors, making it difficult for doctors to accurately interpret new findings. Additionally, aggressive company advertising may lead to the overuse of expensive brand name medications, driving up costs and exposing patients to the risks of newer, less studied drugs.
The media can help counter these commercial influences by identifying bias in medical research and by presenting information in an even-handed manner. In this week's issue of the Journal of the American Medical Association, however, we report the results of a study suggesting this does not always happen.
We reviewed 300 recent news articles about medication studies - all funded by pharmaceutical companies - and found that 42 percent neglected to indicate the funding source. As a result, readers were left in the dark about an important source of study bias. Additionally, 67 percent of the articles referred to medications by their proprietary brand names - rather than the generic names - unnecessarily commercializing the scientific findings and perhaps promoting the use of costly brand name drugs when older and better-tested generics would be as good. Our study is not the first to raise concerns about news coverage of medical therapies. Previous research has suggested that news reports commonly overemphasize the benefits of treatments, fail to discuss their side effects, and exaggerate their uses.
Many factors may explain these shortcomings. For example, there may be a desire of journalists to make their stories upbeat and absorbable. A more concerning possibility, however, is that journalists are influenced by pharmaceutical promotions. We were reassured to discover that just 4 percent of 100 newspaper editors we surveyed had accepted a gift from a company representative within the past year. Still, pharmaceutical representatives frequently send journalists favorable press releases and other materials that are not balanced by alternative views. Journalists also interact with pharmaceutical representatives at medical conventionsJournalists may also promote commercial interests at the expense of scientific and social ones by failing to serve their watchdog function. They may neglect to indicate when a study has received company funding because they are not aware of the funding source or do not think it is important. Similarly, they may refer to medications by their brand names because they do not know which names are which or do not realize that the use of brand names can lead to irrational use of costlier drugs.
In response to concerns about growing commercial influences in medicine, the Association of Health Care Journalists recently published a Statement of Principles that calls on medical journalists to "investigate and report possible links between sources of information and those who promote a new idea or therapy." The Principles also exhort journalists to "report the complete risks and benefits of any treatment, along with the possible outcomes of alternative approaches."
News organizations should implement and enforce these guidelines, ideally with two additional stipulations:
* All articles concerning medical research should indicate the funding source and should note whether quoted experts have financial ties that might influence their opinions.
* All articles concerning medical research should refer to medications by their nonproprietary generic names.
The medical community has a responsibility to help journalists comply with these stipulations by ensuring that medical journal articles and press releases about research emphasize commercial influences that may have biased the findings. Journal articles and press releases must also refer to medications predominantly by their generic names, and emphasize the limitations of new therapies. If doctors and journalists work together to reduce commercial influences in medicine, it will result in better informed clinical decision making.
-
Dr. Michael Hochman is an internal medicine resident at the Cambridge Health Alliance. Dr. Danny McCormick is a primary care physician at the health alliance and assistant professor of medicine at Harvard Medical School.
-
---------
"Long Term Health Care: Health care gobbling up NH paychecks"
By TOM FAHEY, State House Bureau Chief, The NH Union Leader (Online), 10/08/2008
CONCORD – Health insurance costs in New Hampshire climbed nearly five times faster than paychecks, a national study has found.
At the same time, benefits in health packages are being trimmed and co-payments for services are going up, according to a new study by 2008 Families USA.
Health insurance premiums between 2000 and 2007 went up 79 percent, while the average worker's earnings rose 16 percent, the group found. During that time, the cost of the average employer-sponsored family plan went from $7,525 to $13,460, an increase of almost $6,000, the report found. Findings were based on data compiled by the Medical Expenditure Panel Survey at the U.S. Department of Health and Human Services.
Compounding the spike in premiums is the fact that employers are shifting costs onto workers. The share paid by employers went up 72 percent while worker costs doubled, climbing 101 percent, Families USA Executive Director Ron Pollack said.
"What's so surprising about these numbers is that these premiums now purchase thinner coverage -- fewer benefits, higher deductibles and co-payments on company-provided insurance," Pollock said. "People are paying more and more and they are receiving less and less."
The report came out one day after a New Hampshire Center for Public Policy Studies report found insurance costs eat up 15 percent of the average family's income.
Personal health care costs of all kinds consume 18 percent of the state's economy, more than $10 billion annually, nearly double their share of the economy 20 years ago.
If the trend continues, health care will consume between 22 and 25 percent of the state economy in 20 years.
Spending at hospitals in 2007 alone totaled more than $3 billion, the study found.
Dennis Delay, deputy director of the center, said that the state needs to rein in the increases, yet faces an economy in which roughly one in nine jobs depend on the health care industry.
"Health care is an increasingly important part of economic activity. So as we move to control health care costs, it means that one of New Hampshire's primary economic engines will have to be controlled," he said.
The Center study also found that New Hampshire workers pay about a quarter -- 26 percent -- of the cost of their health care. Employees paid 23 percent of the cost in 2000.
Pollock said New Hampshire's experience is close to the national average.
He said some solutions would be to let the government negotiate drug prices for Medicare clients, boost the use of information technology to reduce expensive medical errors, shift payments toward the most effective and cost-efficient therapies, and emphasize preventive and coordinated care.
-
Readers' COMMENTS:
I have to say, I am impressed by the UL's move to articles that affect us all. Even more impressive is the quality of the comments. I learned some things from these informed posters. While traffic accidents and who gets hired or fired in a little town hall is interesting, it doesn't really warrant front page news. If the UL posted more info on the economy, health care the elections, who knows, your online site might just thrive. Let's see some follow-up on this subject UL...it is a front and center for us all. Thanks!
- Cathy McDonald, Derry, NH
we are currently without health insurance. My husband just switched jobs as the company he was working for had slowed down enough that a layoff was looming so he figured he'd better move on while he had a chance to. We had a choice - have health insurance or pay the bills.
Luckily we are both healthy middle-aged, or so, people.
And no option available. We got the COBRA paperwork the other day $1,300/month for family coverage. ONE THOUSAND THREE HUNDRED DOLLARS!!! I don't even make that a month.
If I took the plan where I work I would owe my boss $50 every week, not have a paycheck with a $2000 deductible and a $30 copay!!!
It's nuts....But I read not too long ago that insurance companies had a huge profit this year. Chances are good their COEs are at the spa with AIG getting more ideas on how to stick it to us
- Mary, thornton
To Zizzy and Ritchie,
While lack of exercise and eating habbits play a large factor in the overall health of people it is not the be all and end all of the problem here. Some people need health care due to injuries, some have health issues that are hereditory, and some are age related. I think Rob in Manchester brought to light a point that needs to be explored. Why aren't there more insurance companies allowed to sell health care policies here in NH. It is my understanding that currently only 4 insurance companies are allowed to sell health care polices in NH. Why is that? Who's palm's are being greased here? I personally have not needed togo to a doctor except for my once a year physical, yet the insurance premiums for my health care or exorbitantly high. It seems to me that if there were more competion in the healthcare market we could see some of these costs coming down.
- Roger, Manchester
A la carte=increase in premiums. As with any "a la carte" system the companies set a lower rate but once you combine all the rates amazingly you are higher than the plan not "a la carte". Why, for example: only a certain % use the chiropractic care so that's $25/month premium now but with a la carte only the people using it take that option so it's $100 per month now etc.... etc.... A La carte is the opposite of where things need to go, it makes lower rates for some and higher rates for other ehich equals more unisured people which mean higher hospital costs and thus even higher premiums than now in the end.
That health care, a basic need, is for profit is crazy thinking to begin with. Regulation on the pricing end of things is what's needed.
We spend twice the amount of money than other industrialized nations and every independent study shows we rank toward the bottom in overall health care.
JAC from Manchester has some real points, a great starting point in minimizing the health care increases(twice as much as inflation). Those points made by JAC seem to be no brainer things that should be done ASAP and start us on a road to clean up a disaster.
- Kevin, Derry NH
You mean the insurance companies are taking more money than they need? WOW! What a shock! Next we'll read about CEO's from investment firms stealing money! Oh, wait!
- scott, chichester
I found it interesting how many of you had the same experience with Harvard Pilgrim that I had. Two years ago our company switched to Harvard Pilgrim because the premiums were similar to the plan we had, with better benefits. The second year, they wanted an out the roof increase for the same coverage. My company then switched to an HRA through Anthem and that seems to be an acceptable choice. Someone mentioned customizing insurance so that you weren't paying for stuff you would never use, like maternity or drug counseling and that sounds like a great idea! A la carte, just like your automobile insurance, just pick and choose what you need (or can afford) and only pay for that.
- Molly W, Manchester, NH
Hey out there you healthy ones, unlike life insurance, no one in this market can be rated so all of us pay for those who don't get out of a chair, eat garbage and pop pills to solve it all. RATE EVERYONE or there will be no incentive to GET OUT OF THE CHAIR.
Secondly, if you look at rising health care costs, college tuitions and housing costs, what is the one common denominator: unlimited availablity of money to the comsumer so the providor or market can increase costs well above inflation. Housing now: declining as funds dry up. College tuition: you watch as they can't raise rates because all these predatory college loan companies won't be able to hand out $40K a year to students sucked into the system. Health care: the only way to stop it is make insurance companies accountable AND rate the user.
Unlimited money causes this - DRY IT UP.
- richie, merrrimack
And yet the empires continue to grow, huge sprawling mega-campuses and buildings. Its a good time to be a 'not for profit' hospital who owns your physicians. Keep it in the family, so to speak. Meanwhile, try finding a primary care physician accepting new patients, or who spends more than 5 minutes with you and is familiar with preventive medicine and screenings appropriate for your sex/age.
Time to spend money getting and keeping people healthy. The system is designed to treat sick people only.
- Zippy, Concord
With obesity rates soaring toward epidemic levels and massive marketing campaigns by the pharmaceutical companies, is anyone surprised by this?
Keep shoving Big Macs down your throat with Anti-cholesterol chasers. Don’t worry, the diabetes will probably kill you before the side effects from the drugs really kick in.
- Zizzy, Manchester
Of critical importance here is to understand that as consumers of health care we do NOT have any control over how our health care dollars are really spent. We "give" all this money to the insurance agency in premiums and anything they pay out is a "profit loss".
The reforms needed are not necessarily needed in health care, but in the financial control of how we pay for it.
Instead of relying on Health insurance companies to "manage" our health dollars, we should individuallly take more control.
Jeanne from Albany paid almost 10,000 for her and her husbands policy....Did they get their monies worth? No way. Perhaps a high deductable policy ($2000) for catastrophic care that kicks in as a regual policy does, and a health savings account with $2000 to spend on the routine maintinance care (screenings, check-ups, other typical medical expenses).
There are faults with HSA's, but if we would allow larger HSA contributions from emplyers to low income employees (and self emplyoed), we may actually be aable to give the advantage of being tax-free conpensation for both the employer AND the empolyee (currently this is not the case as people with no tax burden dont get tax breaks).
An other idea is to allow HSA dollars to be used to pay for the health insurance premiums...this would be a powerful incentive to accumulate money for retiring couples health costs...Fidielity Investments the average retiring couple in 2006 will need $200,000 to cover their health care costs for 20years in retirement (Yikes).
There are other ways as well specific to HSA's, but more importantly, until American take control over THEIR money, and their care, insurance companies will continue to do business as usual. Usually this means HUGE profits and squeezing out a larger and larger customer base.
Also, we need to INVEST in a coordinated and comprehensive Health Education system for our schools putting it on par with Mathmatics and English (higher I hope) in curriculum. If we let our kids learn health via TV and commercials (McDonalds and Viagra) we've got serious issues!
- Seymore, Manchester
Having worked for a few health insurance companies in NH for many years, I have some ideas. There are many areas that drive up the cost of health care; my focus at the moment is in the insurance side of things. It is time to change the way health insurance works to reduce costs of administering it.
1) Mandated insurance regulations need to be standardized across the country. It is extremely expensive to for an insurance company to start doing business in another state because all of their systems, policies, procedures, etc. have to be modified for each state. All of their employees have to be retrained for additional states. They need to go through extensive audits for each state. Yes regulate, but simplify at the same time.
2) Get rid of the concept of networks. Insurance companies dictate who can practice medicine in a particular area. If there are three primary insurers in a state, and two of them tell a doctor that their network is "closed" and not accepting new providers in that area, that doctor is out of business and has to go work for one of the in-network providers. At the same time, patients in that same area often have difficulty finding an available provider who is in-network. Big practices who are also in-network have too much influence over insurance companies to pressure them to not allow any new providers in their area. The concept of networks are anti-competition in the health care field.
3) Once networks are gone, level the playing field by requiring insurance companies to pay all providers the same (fair and reasonable) dollar amount for a particular service (CPT code). The insurance company posts their payment schedules, providers post their fee schedules. From that, patients can decide which insurance plan they want to buy, and they can also decide which doctor they want to see, knowing that they'll be paying the difference between the payment and the fee charged. If a patient wants to go to a world renowned doctor for a particular type of service, that doctor will get paid the same amount as the guy down the street, and the patient will pay the difference to the doctor for the luxury of selecting someone who is much more expensive. That is how the fair market, competition, and consumer choice works in America!
- JAC, Manchester
The company I work for uses the same health care provider as Jeanne from Albany, NH. We had to switch from Anthem Blue Cross Blue Shield because of their ever increasing high rates. I feel that we were lured in by Harvard Pilgrim because for the first year with them we did pay less than with Anthem, but just for the first year! We had a $15.00 co-pay for doctor visits with a $500.00 individual and $1,250.00 family deductible maiximum, "same as with Anthem" and as I said the premium was lower. However at renewal time beginning our second year with Harvard Pilgrim our premiums jumped 7,000 and our deductible jumped to $1,000.00 per individual and $3,000.00 from the family deductible and our co-pay is now $25.00 for doctor office visits. Our boss tried diligently to shop around for the same health care coverage at approximately the price we were paying for the first year with Harvard Pilgrim, but guess what? The number of insurance companies that are authorized and can sell health care policies in NH is very limited! I have to wonder why this is? Why can't more insurance companies sell health care insurance in NH? I think that competion would help keep prices down. These increases in health care costs this year ate up any chances for bonuses from a profit sharing program that our company had done for all employees in previous years, as well as eliminate any possibility of raises. Unfortunately due to health problems that both my wife and I have we don't have the luxuary option of dropping our health care insurance to save money. With higher prices for everything from heating fuel, groceries, gasoline, coupled with taxes going up and the shrinking value of the dollar, I fear it won't be long before we all go from our current economic crisis situation to a situation where nobody can afford to survive. I am seriously concerned how I'm going to heat my home this year and till but our medications!
- Rob, Manchester
The piece of this puzzle that rarely gets mentioned is that every time the NH legislature adds another requirement - the cost to the consumer goes up. Many of the uninsured would gladly purchase a lower cost policy that didn't include maternity, drug rehab, chiropractic services, mental health coverage, etc. if it made the cost more affordable.
Individuals should also be able to pool with other people to create groups similar to those currently only existing via their employer. Think about it - why is anyone's employer the one who determines which health insurance coverage they will have?
I would love to see NH set an example for the rest of the country and work outside the box for innovative ways to reduce the cost of insurance and make insurance less connected to employers. Combine this with making the actual costs for medical care more transparent so that people know ahead of time how much they are paying for a particular service.
- Tammy, Manchester
A well timed and placed article... What a coincidence!
- Mike W, Milton, NH
My husband and I carried insurance through his vacuum repair business; only two of us on the policy. The premium was 813 a month (a hardship)for the first year. Imagine our shock when our premium increased to 1,300. a month the second year! After putting pressure on a rep. from the insurance company to explain this, she confessed this type of policy was no longer cost effective for the company and they were phasing it out. How sick would my husband become struggling each month to come up with an extra 500. a month for healthcare? We chose to cancel the policy, of course, and joined the ranks of the uninsured. The company was Harvard Pilgrim Health, by the way, so watch out.
- Jeanne Kukuruza, Albany, NH
---------
"Worse health care: Obama's costly mandates"
The New Hampshire Union Leader, Editorial, Thursday, October 9, 2008
Health care costs are rising everywhere. In New Hampshire, they account for 18 percent of the state economy, according to a new study by the New Hampshire Center for Public Policy Studies. And a study by the left-wing Families USA says they rose five times faster than incomes in New Hampshire since 2000. What is to be done?
Barack Obama's answer is to regulate. He proposes forcing businesses to offer health insurance plans that meet as-yet unidentified government standards. If they don't, they'll be fined by having to pay a percentage of their payroll to the government (Obama won't say how much). Obama also will force insurers to spend more of their premiums on care instead of keeping them for profits or administrative costs.
This will force insurers to hire lots of bureaucrats to do paperwork. But administrative costs already account for 31 percent of existing health care costs in the United States, according to a study in the New England Journal of Medicine five years ago.
The more government tells insurers what to do, the more insurance costs. As Sen. John McCain pointed out in Tuesday night's debate, Americans are forced by states to buy insurance that covers things they don't need. Seven states require all insurance plans to cover hairpieces. That's crazy. And it drives up costs for everyone. Studies have shown that insurance costs less in low-regulation states than in high-regulation ones.
McCain proposes increasing market competition to drive down prices. He would reduce government mandates, and let people buy health insurance much like they buy car insurance. That's a lot better than more government mandates of the kind that have made health care so much more expensive than it has to be.
READERS' COMMENTS:
Chris from Bedford, the equation the labor market eventually solves is my benefit to my employer versus his cost to employ me. If part of my employer's cost to employ me is removed, the labor market will eventually let me negotiate higher pay, as my value to him and his cost would not change. We often note that the "employer-paid portion of social security" ultimately comes out of the employee's pocket for this very reason.
McCain's plan would indeed discourage health insurance as a job benefit and encourage individuals to buy it out of a fatter paycheck. For the reasons of individual control I gave earlier, this seems like a good thing. The fact that the fatter paycheck is taxed is not a McCain invention, and Obama is stretching to describe this secondary effect of a secondary effect as though McCain dislikes wage-earners.
- Spike, Brentwood NH
We are supposed to be so very proud that the ruling class has great coverage, the best medical attention, fanciest procedures, finest in the world. Trouble is working folks can't break into the ruling class!
Like national defense, health care is a top national priority - period. That means we have to figure a way to get the most people affordable adequate coverage.
The phony free marketeers want the same type system that distributes money for home loans - a capitalist Wild West free for all. But health care is too important to let it be all about profits. Insurers will always make money, don't worry about insurers! The question is will our health suffer in the process?
- Claire Collins, Hanover
I've been saying the same things for years ,Doug. Unless the cost of an x-ray for example is lessened how can health insurance cost less. What we need are tighter reins approving licenses for doctors and in turn, hopefully, driving down their liability insurance. I would rather see doctors in private practice than to deal with these large health care facilities.
- laurel667, manchester
Don,
You base your argument on a very tenuous premise, that the money your company pays for your health care will be given to you in cash when they stop paying for your health care.
My company pays 10K of my healthcare and if they stop the coverage, I would not count on having an increase in salary of 10K.
Also, companies are able to negotiate lower rates than an individual. A company can negotiate better rates by saying we will insure 100+ employees through so and so health plan. If you are alone, you have no negotiation ability becasue you are just a small fish.
- Chris, Bedford
Carlos, I am one of your "45 million" uninsured. I don't buy first-dollar coverage but buy Major Medical. For the small stuff, rather than whine that something isn't my fault and that a stranger should pay, I pay cash out of pocket and I get the treatment I want. This is preferable to becoming a patient of the United States. People with "free" health care (veterans, Cubans, Canadians, Brits) like the institution but don't like their care, nor the fact that their only recourse is to write their legislator.
And, Carlos, health care IS "available for all Americans." Every hospital has to treat everyone, notably foreign invaders, regardless of ability to pay. That's why those of us who can pay, pay exorbitant prices. That's what partial socialism gets you. Complete socialism doesn't work any better. So spare us the appeals to pity.
- Spike, Brentwood NH
This editorial completely ignores reality, which is that despite spending more than any other nation in the world, we have the highest percentage of uninsured people among industrialized nations. Countries that have socialized medicine pay less, cover more people and are generally healthier than in the US. Plus, American companies face a significant competitive disadvantage over foreign competition because they have to subsidize health care costs for their employees while their competition does not.
Not surprisingly, the UL has ignored all of this evidence simply because it doesn't like Democrats. And it wonders why it has lost any influence it may have once had.
- Jason, Londonderry
Cory, so what. If in the end everyone who has health care coverage now, has health care coverage then, what does it matter if my employer is involved? Realize I'm not saying that that is what will happen with McCain's plan.
My boss is an idiot. I wouldn't allow him to clean up after my dog. But guess what, he's one of the people who negotiates my company's health benefits. Lucky for me there are a couple of smart people who do as well to offset his idiocy.
Maybe if we could stop some of the lawsuits that only serve to line lawyer’s pockets, the cost of health care would start coming down and you and I could afford to buy what ever coverage we wanted. Then we would be beholden to anyone for our health care choices.
- Dan, Nashua
Cory-
Should your employer pay your auto insurance? Please explain why your employer should have to pay for your health insurance.
- Tyler, Farmington
Whats wrong with eliminating employer based coverage? Does your employer offer you auto, home, or renters insurance? Getting the employers out of offering insurance will drive up income and create jobs, and at the end of the year get a nice credit to either cash out or reduce your tax bill. Letting us buy health insurance (like we do with auto) across state lines will also reduce costs as we wont be forced to buy only from a few providers. Cory, last time i checked all of those state socialized medical programs in NY weren't doing so well and services were being rationed to those enrolled. All Obama wants to do is to "crowd out" the insurance companies and stick americans with a hefty tax bill.
- Don Rubby, Exeter, NH
No one can drive down (or even reduce the rate of increase in) health insurance costs without driving down the cost of the medical services themselves.
The reality is that an insurance company figures out how much it will have to pay out in claims, then adds in its advertising, claims processing, and administrative costs and a 5-6% net profit. The net result is that insurance companies need to take in about 15-17% more in premiums than they pay out in claims.
If the dollar cost of claims increases 10%, then premiums will rise about 10%.
Politicians who claim to have a solution to increasing health insurance costs are crazy if their proposal does not include tight caps on what health care institutions (doctors offices, hospitals, rehab centers, drug manufacturers, outpatient clinics, labs, etc.) can spend. Why? Because you can be sure that whatever they spend they will charge in claims to the insurance companies. Those companies will simply pass those charges on with their 15-17% premium for being the middleman.
- Doug, Chichester
Neither plan addresses the issue of making health care available for all Americans. Right now there are 45 million Americans who don't have any coverage at all. It is estimated that 18,000 people die each year because they don't have insurance. What is the cost of 18,000 lives?
- carlos, francestown
What the UL fails to do in this editorial (not surprisingly) is to state what John McCain's untimate health care goal is: the elimination of employer-based coverage.
- Cory Taliaferro, Albany, NY
---------
-
www.boston.com/bostonglobe/editorial_opinion/oped/articles/2008/10/22/breaking_the_cycle_of_waste_in_healthcare/
-
---------
"Court rejects cap on Medicare rates: White House sought 'least costly alternative'"
By Robert Pear, New York Times News Service, November 4, 2008
WASHINGTON - A federal court has blocked the Bush administration's effort to save money on Medicare by paying for only the least expensive treatments for particular conditions.
Congress sets Medicare payment rates and never intended to give officials broad discretion to alter them, the court said in an important test case last month.
The case, closely followed by Medicare officials and consumer advocates, involved drugs used to treat chronic obstructive pulmonary disease.
Judge Henry H. Kennedy Jr. of the US District Court here said the policy of paying for only "the least costly alternative" was not permitted under the Medicare law.
The administration's position would give the health and human services secretary "enormous discretion" to determine the amount paid for every item and service covered by Medicare, without reference to the detailed formulas set by Congress, Kennedy said. "This flies in the face of the detailed statutory provisions," he added.
Over the years, Medicare officials have often tried to adopt regulations that allow them to consider cost in deciding whether the program should cover various goods and services. Health care providers, manufacturers and some patients' advocates have resisted these efforts, saying that coverage decisions should be made based on clinical effectiveness and not cost.
"We are disappointed with the ruling and continue to believe that our policy is supported by the statute," Peter L. Ashkenaz, a spokesman for the federal Centers for Medicare and Medicaid Services, said yesterday. "We are still considering our options and next steps."
Federal health officials said the decision would make it more difficult to rein in Medicare costs.
Kennedy found that Medicare and some of its contractors had unlawfully limited payments for DuoNeb, an inhalation drug taken through a nebulizer, which turns the medicine into a fine mist.
The drug, made by Dey, a unit of Mylan Inc., makes breathing easier by opening up the bronchial tubes. A single dose provides a combination of two commonly prescribed bronchodilators, albuterol and ipratropium.
Congress set forth the touchstone for Medicare coverage in a 1965 law that created the program. The law generally prohibits payment for items and services that are "not reasonable and necessary for the diagnosis or treatment of illness or injury, or to improve the functioning of a malformed body member."
If an item is covered, the payment rate is specified in other parts of the law.
The Bush administration argued that Medicare officials had the right to decide whether the expense incurred for a given item, not just the item itself, was "reasonable and necessary."
---------
The Boston Globe, Op-Ed, DERRICK Z. JACKSON
"Gender equity a premium for healthcare"
By Derrick Z. Jackson, November 4, 2008
IF BARACK Obama or John McCain wants to bring Americans together after the presidential election, there is one proposal that could unite voters across the country. The winner of today's election should pledge to end gender discrimination in health insurance for women.
In a recent report, the National Women's Law Center found that women - both young and middle-aged - pay dramatically more in most states for individual health insurance than men. Only 12 states offer gender discrimination protection, only eight offer protections for age and only 15 offer protections for health status. According to the report, insurers in nine states and the District of Columbia can legally reject applicants who are survivors of domestic violence. In many states, insurers can reject women simply for having undergone caesarean sections in the past.
The severity of the problem differs from state to state and from age group to age group. The report lists nine states where a 25-year-old woman would pay from 38 percent to 45 percent more for individual coverage than men of the same age. And the report lists 27 states where a 40-year-old woman might pay from 37 percent to 48 percent more for coverage.
Refreshingly, the rules are more equitable in most of New England. Massachusetts, Maine, New Hampshire, and Vermont all either prohibit or significantly limit gender discrimination in the issuance of individual policies. The report specifically cited Massachusetts' effort to decrease costs and increase the number of plans available by merging individual and small group markets into one large pool. Pooling the markets allows for spreading risk more broadly and cutting bureaucracy. "This model could be adopted by other states, or it could be applied nationally by the federal government," the report said.
Three-quarters of the nation's women are largely protected from gender discrimination in health insurance, as they get it either from their employers or through public programs. Meanwhile, 18 percent of women have no insurance at all, and 7 percent have individual plans. Taking the gender gap out of health insurance policies may make them far more attractive to the 18 percent without insurance.
Insurers have all kinds of excuses for discriminating against women. In The New York Times, a senior vice president of Humana, Thomas Noland Jr., said, "Premiums for our individual health insurance plans reflect claims experience - the use of medical services - which varies by gender and age. Females use more medical services than males, and this difference is most pronounced in young adults."
Noland went on to say, "Bearing children increases other health risks later in life, such as urinary incontinence, which may require treatment with medication or surgery."
Noland's bland explanation cannot hide the Neanderthal implications. Humana's sense of humanity is incontinent. This thinking punishes women at least twice, once for simply having children and again for simply taking better care of their health by seeing doctors more regularly than macho men who wish away the pain in their chests until the surgeon is cutting them open in the operating room.
The president of the National Women's Law Center, Marcia Greenberger, said that there is no justification for this kind of discrimination, likening it to using race as a factor.
The winning presidential candidate should incorporate the report's finding into his healthcare plans. McCain has promised high-quality coverage to people "who have the most difficulty on the individual market." His $5,000 tax credit to purchase insurance would be worth less to women in most of the states. Ending gender discrimination would be crucial to making such a tax credit fair.
For Obama, who said he will require insurers to cover preexisting conditions, the report represents an immediate opportunity to show supporters of Hillary Clinton, who many specialists said had the best healthcare plan of all the candidates, that he takes them and women's issues in general seriously. Obama says he understands that women "continue to shoulder substantial economic burdens."
Regardless of who wins today, unfair health insurance costs should be one of the first burdens the new president lifts off women's shoulders.
-
Derrick Z. Jackson can be reached at jackson@globe.com.
-
---------
"Extortion Used in Prescription Data Breach: FBI Investigating Threat Against Express Scripts Customers"
By Brian Krebs, washingtonpost.com Staff Writer, Saturday, November 8, 2008; D01
One of the nation's largest processors of pharmacy prescriptions said this week that extortionists are threatening to disclose personal and medical information about millions of Americans if the company fails to meet payment demands.
St. Louis-based Express Scripts said Thursday that in early October it received a letter that included the names, birth dates, Social Security numbers and, in some cases, prescription data on 75 of its customers. The authors threatened to expose millions of consumer records if the company declined to pay up, Express Scripts said in a statement.
Chief executive George Paz said in the statement that Express Scripts has no intention of paying and that his company is working with the FBI to track down those responsible for the scam.
Express Scripts is the third-largest U.S. pharmacy benefit management firm, which processes and pays prescription drug claims. Working with more than 1,600 companies, it handles roughly 500 million prescriptions a year for about 50 million Americans.
Express Scripts has notified its clients of the threat. Fairfax County Public Schools yesterday sent a letter to employees alerting health-plan participants who use Express Scripts to the breach.
"FCPS is deeply concerned about this kind of breach, which could adversely affect our employees," Superintendent Jack D. Dale said in the letter. "We expect and deserve the highest level of security when we entrust our vendors to handle our employees' personal information."
The letter was delivered by mail, said company spokesman Steve Littlejohn. He declined to say how much money the extortionists were demanding. He added that the company is trying to determine how the data were stolen.
"We know where the data came from by looking at it, but precisely how it was accessed is still part of the investigation," Littlejohn said.
The company last week set up a Web site to give consumers tips on how to protect their identity. While Express Scripts does not interact with consumers directly, the company's name is printed on prescription cards of health-care plans that use its services, Littlejohn said. The 75 people listed in the letter have been notified.
Billy Cox, special agent for the FBI's St. Louis field office, confirmed that the bureau was contacted by Express Scripts, but declined to comment on the case.
Alan Paller, director of research for the SANS Institute, a Bethesda-based computer-security training group, said many companies, especially in the financial industry, have already paid to keep their customers' data from being released. Some receive more than one extortion threat a day.
Paller said that in some ways, the health-care industry is the perfect target.
"Nobody is going to want to go to a health-care provider if they think their private medical history is going to be revealed to the world online," he said. "Hospitals wouldn't have to think too hard about that before paying off an extortion demand."
Last month, the FBI arrested an Indiana man accusing him of stealing 900,000 policyholder records from a medical provider and trying to extort $208,000 from its parent, American International Group.
Graham Cluley, a senior technology consultant for Sophos, a British computer security company, said Express Scripts was right to go to the FBI.
"Data extortion is not like if your daughter gets kidnapped: Even if something is returned to you, you can never be sure they're not going to carry on taking advantage of the situation," Cluley said. "The bad guys can always just make a copy of what they've stolen, and they can keep on coming back and asking for money, or they can still go and sell the data online."
---------
"A day of dental health care for all: Program 31 sponsors free clinic next weekend"
By Trevor Jones, Berkshire Eagle Staff, Monday, November 10, 2008
PITTSFIELD, Massachusetts — For those who hate making a trip to the dentist's office, there may be one less reason to worry.
Project 31, a program established by the International Team of Implantology, will be holding a free dental clinic in Pittsfield on Saturday, Nov. 22, at the office of the Oral Surgery Associates at 3 Dalton Avenue, to remove teeth and put in fillings for anyone who shows up.
Dr. John-Michael Stewart, a dentist and oral surgeon who has an office in Pittsfield, is the northeast representative for the International Team of Implantology which established the program. He said the program can help the growing number of people who can't afford dental care.
"Especially with the (state of the) economy, people cant afford the luxury of regular cleanings," said Stewart adding that with more dentists retiring than entering the field, it has become increasingly difficult to get an appointment as well.
"This is for people who just can't do it on their own," he added.
This will be the second program the organization has offered, the first being in Wilmington, Vt. in August. That day Dr. Stewart and his associates serviced 250 people, receiving $170,000 worth of free services. Stewart said the program was such a success they decided to offer a second clinic before the year was out and chose Pittsfield with the hopes of an even greater turn out.
Sponsored by the Pittsfield Rotary Club, Berkshire Medical Center and Guardian Life Insurance, Stewart said the program has received strong backing locally.
"There has been tremendous support. The community really seems to be liking the idea of free dental care," said Stewart.
With 12 dentists from around the state working and twice the office space as was available in Vermont, Stewart has set a goal of provide more than $250,000 worth of free care with the potential of making the clinic a a semi-annual event.
Project 31 — named for the 31 million people across the country who don't have access to dental insurance — is first-come, first-served and there will be no restrictions for those seeking help.
People are asked to check in at the Dalton Avenue location, where tooth extraction will take place. Those who are determined to need fillings will be bussed to the office of Dr. John George on Tyler Street.
Stewart said taking proper dental care is important not only in maintaining one's teeth, but for people's overall health. He pointed to studies which showed that bacteria found in untreated teeth can get into the bloodstream and lead to diabetes, heart and kidney problems.
Beyond a person's health, Stewart said the program makes everyone involved feel better about themselves.
"If I can help them save a tooth by giving free care, it makes me feel good and it makes them feel good by knowing they have the confidence to smile."
-
Trevor Jones can be reached at (413) 528-3660 or tjones@berkshireeagle.com.
-
If you go ...
What: Project 31, a free one-day dental clinic, with extraction and basic restorative dental care by local dentists and oral surgeons on a first-come first-serve basis.
When: Saturday, Nov. 22, 8 a.m. to 4 p.m.
Where: The offices of Oral Surgery Associates, 3 Dalton Avenue, Pittsfield.
---------
The Boston Globe, EDITORIAL, Short Fuse, November 12, 2008
"Medicaid: Skimping at exactly the wrong moment"
Just as President-elect Obama and Congress push for increases in the federal share of Medicaid to relieve beleaguered state budgets, the Bush administration has put in place a new rule that will cut Washington's contribution to the healthcare program. Last Friday, the administration announced it would narrow the scope of outpatient services that hospitals can provide to Medicaid recipients, including some dental and vision care. During its November lame duck session, Congress should put a moratorium on the rule, which goes into effect Dec. 8, and one of the first acts of the Obama administration should be to withdraw it.
---------
"Senate Democrats move on healthcare"
Posted by Foon Rhee, deputy national political editor, The Boston Globe Online, November 12, 2008, 1:00 PM
A key Senate Democrat unveiled a healthcare reform plan today -- the first move by congressional Democrats to push President-elect Barack Obama to move on the issue quickly after his inauguration.
The proposal from Finance Chairman Max Baucus of Montana -- whose staff has reportedly been working for months with the staff of Senator Edward M. Kennedy, of Massachusetts -- echoes key elements of Obama's campaign proposals, including expanding Medicaid and the children's healthcare program. It also is similar to the landmark plan in Massachusetts.
But like the plan offered by Obama's former rival, Hillary Clinton, it requires people to get coverage while offering subsidies to those who can't afford it. Obama didn't include the individual mandate in his campaign proposals, saying it was more important to make coverage affordable so that people would get it without a requirement.
Baucus told reporters that he talked to Kennedy this morning, and while he wouldn't disclose the conversation, he suggested they are on the same page.
While Obama will likely be focused on the economic recovery when he takes office in January, a broad coalition of groups want him to use his honeymoon to make progress on healthcare as well.
As the New Republic magazine notes this week, some of the same business groups that helped kill the last major attempt at universal coverage during the Clinton administration 15 years ago now support reform, in part to control rising costs that are sapping the competitiveness of US companies.
---------
The Boston Globe, Op-Ed, JIM GOMES
"Healthcare, education through the looking glass"
By Jim Gomes, November 17, 2008
TRANSITIONS are exciting times, buzzing with possibility and new ideas. Task forces, academics, and bloggers seek attention and support for their reform proposals, dreaming things that never were and asking, "Why not?"
Many people believe that American education and healthcare are overdue for reform. However, meaningful change is unlikely unless we recognize the irrational elements of both systems, flaws we may not even notice because we have become accustomed to them.
A thought experiment may be helpful: What if public education worked like our healthcare system?
First, children's education would depend on where their parents worked. If the employer provided it as part of a benefits package, kids would receive an education. Some employers would offer high-quality educations to their employees' kids, while others would offer stripped-down schooling that omitted whole subjects or stopped after sixth grade. Students would bring daily co-payments to school with their lunch money.
America would also have a program for poor children whose parents did not have jobs or had jobs without education benefits. However, the quality of education would vary widely depending on how much funding each state provided. One child in seven would have no education plan at all, although they could receive instruction on an emergency basis - for example, just before the SAT exams.
Teachers would be paid in piecework fashion, their compensation depending on how many lessons they taught each day. Much of the nation's education budget would be spent determining whether students' educational payment plans covered a particular subject, and on TV ads pushing new materials for teaching various subjects.
Of course, no one is proposing that public education emulate our healthcare system, and for good reason. It would strike most people as wrong-headed to tie the availability and quality of kids' schooling to their parents' jobs. We would quickly see that paying teachers by the lesson creates the wrong incentives. We wouldn't stand for all the haggling, delay, and administrative cost of deciding whether a benefits plan covered a particular subject.
Yet we tolerate just such bizarre arrangements in our healthcare system. Tens of millions lack access to care. Doctors get paid to do procedures, not to get or keep people healthy. Insurance companies waste untold billions playing the "your plan doesn't cover that" game.
So, now imagine if American healthcare worked the way our education system does.
The three most important factors in the quality of your healthcare would be "location, location, location." Adjoining towns or counties would have dramatically different levels of care and health outcomes. Young couples would stretch their budgets and lengthen their commutes to live in communities with the best doctors and hospitals.
After doctors had practiced for three years, they would become tenured. But they would receive only modest salaries, and our most promising young people would choose different careers. Many doctors would not be able to pass exams in anatomy or physiology, but all would have taken the required course in theories of medicine in order to be certified.
This is not a world most of us would want to live in. Yet we do - it's the world of American K-12 education. Access is universal, but quality varies widely and is often poor.
Both systems are deeply flawed, but their weaknesses and irrationalities can be hard to see simply because we are so used to them. Flip them, and it's easier to recognize their problems.
In the real world, of course, healthcare and education have a few things in common. Both doctors and teachers resist being evaluated or paid based on the outcomes achieved by their patients and students, claiming that it is unfair or too complicated to sort out their own contributions to results. Poor people and people of color get disproportionately bad outcomes from both systems. And, of course, the wealthy can buy their way out of either, choosing "concierge medicine" or elite private schools.
Reforming these critical sectors will not be easy. But our economic competitiveness, quality of life, and basic fairness all make change imperative.
-
Jim Gomes, a guest columnist, is the director of the Mosakowski Institute for Public Enterprise at Clark University.
-
---------
The Boston Globe, Op-Ed, MADELINE DREXLER
"The need to combine social and health policy"
By Madeline Drexler, November 18, 2008
-
First in an occasional series giving advice to the new president.
-
SINCE THIS is, by all accounts, a "defining moment" in American history, let's redefine the way we think about health. Over the past decade, a rich vein of research has detailed the links between large social forces - from income and discrimination to education and neighborhood safety - and a community's physical and mental well-being.
Last summer, a pair of fascinating reports - overlooked in the US press - drew on this perspective to suggest a blueprint for the next administration's health agenda. Both reports stepped back from our conventional explanations of health - "individual lifestyle" and "biomedical miracle" - to analyze the structural factors behind disease and suffering in our society.
"The Measure of America," published by the Social Science Research Council, an independent research organization based in New York, examined US health through a novel lens: the human development model that the United Nations has applied around the world - but, until now, never to the world's richest and most powerful country.
Underscoring how far we lag in our promise, the report documented how the roughly $5.2 billion we spend every day on healthcare yields a pitiable return on investment. For example, US life expectancy ranks below that of Chile, Costa Rica, and nearly every European and Nordic country. The US infant mortality rate is on par with that of Croatia, Cuba, Estonia, and Poland. Within the United States, stark health inequities persist along socioeconomic and racial/ethnic lines.
What's behind these dismal facts? Not just sedentary habits or calorie-laden diets, although obesity is a major factor in America's relatively faltering position. Rather, it's how public- and private-sector priorities shape health. As the other groundbreaking document - the World Health Organization's final report from the Commission on Social Determinants of Health, "Closing the gap in a generation" - explains: "The unequal distribution of health-damaging experiences is not in any sense a 'natural' phenomenon but the result of a toxic combination of poor social policies and programs, unfair economic arrangements, and bad politics."
And so, the defining moment. If President-elect Barack Obama wants to live up to his ambitious vision, then he must combine social and health policy. First and foremost, push for universal healthcare. "Just like smoking and diabetes, lack of health insurance is an early death sentence," said Sarah Burd-Sharps, a former UN administrator and co-author of "The Measure of America." Every rich nation in the world except ours has figured out how to provide health coverage to virtually every citizen - and at far lower cost per capita.
Next, as do most European and Scandinavian countries, weigh the health consequences of policies in taxation, business development, transportation, housing, agriculture, and so on. Make improving population health and reducing health inequities a criterion for all government initiatives.
Finally, don't use the recession as an excuse not to act. Throughout American history, our bodies have responded well to strong doses of social "medicine." The Depression of the 1930s saw Social Security and collective bargaining - both of which vastly improved health. During the late 20th century, motor vehicle laws, including mandatory seat belts, child seats and lower speed limits, likely saved more lives than anything high-tech medicine offered. According to a 2008 Harvard University study, even the contours of America's entrenched health inequities can change with visionary policy. From 1966 to 1980 - in the wake of the War on Poverty, the US Civil Rights Act, and the establishment of Medicare, Medicaid, community health centers, and the Environmental Protection Agency - US socioeconomic and racial/ethnic disparities in premature mortality and infant death shrank; after 1980, when Republican politics hollowed out the public sector, disparities widened.
In other words, think big. As Dr. Georges Benjamin, executive director of the American Public Health Association, told me during the group's annual meeting last month: "I would love Barack Obama to declare that he wants America to be the healthiest nation in the world - in a generation. Americans need to rally around the idea of grappling not only with healthcare, but with health."
-
Madeline Drexler, a former medical columnist for the Boston Globe Magazine, is a Boston-based journalist and author.
-
---------
"5 Myths About Our Ailing Health-Care System"
By Shannon Brownlee and Ezekiel Emanuel, washingtonpost.com, Sunday, November 23, 2008; B03
With Congress ready to spend $700 billion to prop up the U.S. economy, enacting health-care reform may seem about as likely as the Dow hitting 10,000 again before the end of the year. But it may be more doable than you think, provided we dispel a few myths about how health care works and how much reform Americans are willing to stomach.
1. America has the best health care in the world.
Let's bury this one once and for all. The United States is No. 1 in only one sense: the amount we shell out for health care. We have the most expensive system in the world per capita, but we lag behind many developed countries on virtually every health statistic you can name. Life expectancy at birth? We rank near the bottom of countries in the Organization for Economic Cooperation and Development, just ahead of Cuba and way behind Japan, France, Italy, Sweden and Canada, countries whose governments (gasp!) pay for the lion's share of health care. Infant mortality in the United States is 6.8 per 1,000 births, more than twice as high as in Japan, Norway and Sweden and worse than in Poland and Hungary. We're doing a better job than most on reducing smoking rates, but our obesity epidemic is out of control, our death rate from prostate cancer is only slightly lower than the United Kingdom's, and in at least one study, American heart attack patients did no better than Swedish patients, even though the Americans got twice as many high-tech treatments.
Moreover, the quality of health care is different in different parts of the country. The Centers for Medicare and Medicaid Services have issued a list of 26 measures of quality, such as making sure that heart-attack patients being discharged from the hospital get a prescription for a beta blocker or aspirin to help reduce the risk of a second attack. It turns out that quality is all over the map, and it isn't necessarily better in the places we might expect, such as academic medical centers. Worse still, according to the Congressional Budget Office (CBO), there appears to be no connection between how much Medicare and other payers spend on patients in different parts of the country and the quality of the care the patients receive. You are no more likely to get that beta blocker or aspirin in Los Angeles than in Portland, even though Medicare spends twice as much per beneficiary in Los Angeles.
2. Somebody else is paying for your health insurance.
Nope. Even when your employer offers coverage, he isn't reaching into his own pocket to cover you and your fellow employees; he's reaching into your pocket, paying you lower wages than he would if he didn't have to pay for your health insurance.
Rising health-care costs are partly to blame for stagnant wages. Over the past five years, health insurance premiums have risen 5.5 times faster on average than inflation, 2.3 times faster than business income and four times faster than workers' earnings. Four times. That's why wages have been nearly flat since the 1980s, even as U.S. productivity has been going up. In effect, about half the money you should be earning for being more productive is being sucked up by ever more expensive health-insurance premiums.
If you pay taxes, you're also paying for the health care provided through state and federal programs such as Medicare, Medicaid, the Veterans Administration and the military. All told, the average family of four is coughing up $29,000 a year for health care through taxes, lower wages and out-of-pocket medical expenses.
3. We would save a lot if we could cut the administrative waste of private insurance.
The idea that we could wring billions of dollars in savings this way is seductive, but it wouldn't really accomplish that much. For one thing, some administrative costs are not only necessary but beneficial. Following heart-attack or cancer patients to see which interventions work best is an administrative cost, but it's also invaluable if you want to improve care. Tracking the rate of heart attacks from drugs such as Avandia is key to ensuring safe pharmaceuticals.
Let's just say that we could wave a magic wand and cut private insurers' overhead by half, to what the Canadian government spends on administering its health-care system -- 15 percent. How much would we save? Not as much as you may think. Private insurers pay a little more than a third of what we spend on health care, which means that we'd cut a little more than 5 percent from our total budget, or about $124 billion. That's not peanuts, but it's not even enough to cover everybody who's currently uninsured.
More to the point, we only get to save it once. That's because administrative waste isn't what's driving health-care costs up faster than inflation. Most of the relentless rise can be attributed to the expansion of hospitals and other health-care sectors and the rapid adoption of expensive new technologies -- new drugs, devices, tests and procedures. Unfortunately, only a fraction of all that new stuff offers dramatically better outcomes. If we're worried about costs, we have to ask whether a $55,000 drug that prolongs the lives of lung cancer patients for an average of a few weeks is really worth it. Unless we find a cure for our addiction to the new but not necessarily improved, our national medical bill will continue to skyrocket, regardless of how efficient insurance companies become.
4. Health-care reform is going to cost a bundle.
Only if you think that covering the uninsured is our only priority. Yes, making health care available to all citizens is the right thing to do. But it isn't the only thing to do. We also have to fix the spectacularly wasteful and expensive way doctors and hospitals deliver care.
Our physicians are working within a truly dysfunctional, often chaotic system that prevents them from caring for us properly. Between 50,000 and 100,000 patients die each year from preventable medical errors. According to the Centers for Disease Control, 1.7 million Americans acquire an infection while in the hospital and nearly 100,000 of them die from it. Laboratory imaging tests are routinely repeated because the originals can't be found. Patients with such chronic illnesses as heart failure and diabetes land in the hospital because their physicians fail to monitor their condition. When patients have multiple doctors, there's often nobody keeping track of the different medications, tests and treatments each one prescribes.
Our doctors and hospitals are failing to provide us with care we need while delivering a staggering amount that we don't need. Current estimates suggest that as much as 20 to 30 percent of what we spend, or about $500 billion, goes toward useless, potentially harmful care.
There are two bright spots. One: We can improve the quality of care and cut costs without rationing. There are models out there for how to do it right -- the Mayo Clinic, the Geisinger Clinic in Pennsylvania, the Cleveland Clinic and California's Kaiser Permanente are just a few of the organized group practices that are doing a better job for less. Their doctors are better than average at using the best medical evidence available. They're more likely to be using electronic medical records, which can help keep track of patients who have multiple physicians and need complex care. And they're less likely to provide unnecessary care.
Two: Even moderate reform of the delivery system would improve care and save money. The Lewin Group's analysis shows that a bill proposed by Sen. Ron Wyden, an Oregon Democrat, calling for a more comprehensive overhaul of the health-care system than either McCain's plan or Obama's could actually insure everyone and save $1.4 trillion over 10 years. More reform is cheaper.
5. Americans aren't ready for a major overhaul of the health-care system.
We may be readier than you think. A recent study published in the New England Journal of Medicine found that only 7 percent of Americans rate our health-care system excellent. Nearly 40 percent consider it poor. A whopping 70 percent believe it needs major changes, if not a complete overhaul.
Now is not the time to think small, to cover a few million Americans and leave the bigger job of controlling costs and improving quality for another day. We can't afford not to reform the delivery system as soon as possible. At 17 percent of gross domestic product, health care is the biggest single sector of the economy, and it's consuming a larger and larger proportion every year. According to CBO projections, health care will account for 25 percent of GDP by 2025 and 49 percent by 2082. That's simply unsustainable. Any plan that reforms health care has to do more than simply cover the uninsured. The nation's health and wealth depend on it.
-
brownlee@newamerica.net
-
Shannon Brownlee, a visiting scholar at the National Institutes of Health Clinical Center, is the author of "Overtreated." Ezekiel Emanuel, an oncologist and author of "Healthcare, Guaranteed," is chairman of the center's Department of Bioethics. The views expressed here are the authors' own.
-
---------
-

-
A youtube.com video titled ''Harry and Louise Return'' backs government intervention into healthcare reform.
-
"Lobbies backing health reforms: Insurers change their tune from 1993-94 debate"
By Lisa Wangsness, Boston Globe Staff, December 3, 2008
WASHINGTON - Powerful special interest groups that helped torpedo healthcare reform 16 years ago are now advocating significant changes in the nation's health insurance and delivery system. They are participating in regular discussions about how to expand health coverage and lower costs, key commitments that President-elect Barack Obama made in his campaign.
Significant differences over policy remain unresolved, and even the most optimistic proponents of reform think passing major legislation next year would be difficult. But two key factions, the business lobby and the health insurance industry, are talking seriously about substantial changes that would ideally help cover the nation's 47 million uninsured, improve the quality of care, and tame the growth of healthcare spending.
Today, the nation's largest health insurance lobbying group will present its own proposal for a version of universal health insurance. The group, America's Health Insurance Plans, has put up a website featuring man-on-the-street video interviews of people complaining about the lack of affordable healthcare: "I'm disgusted, I'm frustrated, I don't know what to do about it," a blonde woman with glasses says in one of the interviews. "It's time for the gov ernment to step in."
Leading business lobbyists have also joined in regular negotiations with insurers, healthcare providers, unions and other advocacy groups on what reforms they would support - not just what they would oppose - and they are trying to reach consensus on difficult issues. They have also underwritten television ad campaigns pressing for reform, in cooperation with such unlikely partners as AARP, which represents people over 50, and the Service Employees International Union.
"What's striking this time is the extent to which they're engaging in a constructive way, at least so far, and I think that's very promising," said John Rother, director of legislation and public policy for AARP, which backed President Clinton's failed health reform plan and is again a proponent of reform.
The mood contrasts markedly with the one that prevailed in 1993 and 1994, when the insurance industry sponsored devastatingly effective ads featuring a middle-class couple named Harry and Louise fretting about how Clinton's plan would limit their health choices - "They choose," Harry said. "We lose," Louise agreed - and business lobbies funded an unprecedented campaign against the Clinton plan.
Disagreements persist about how to cover the uninsured, how to control the growing cost of healthcare and how the insurance market should be regulated. But veterans of the Clinton-era health reform efforts say they are nevertheless encouraged by the posture the business and insurer lobbies have struck.
Many who participated in or observed the Clinton health reform efforts say business groups are more comfortable with the process this time - the Clinton reform plan happened through an unusual and secretive process - but next year's legislation appears to be taking shape in Congress, where lobbying groups are comfortable operating.
Chris Jennings, a healthcare lobbyist and former Clinton aide, said that business groups and insurers have more urgent reasons for getting involved this time.
"In stark contrast to '93-'94, their second-best option is no longer to do nothing," Jennings said. "They recognize that a failure to act is an explicit policy choice that has severe and negative consequences to them. . . . This isn't just about altruism."
Business organizations like the National Federation of Independent Business, a small business advocacy organization whose grassroots campaign against the Clinton plan bombarded Capitol Hill with letters and phone calls, say their members can no longer tolerate the rising cost of premiums, which is forcing many small businesses either to stop offering coverage or require employees to pay more for it.
"Our members have continued to say this is their number one issue for 25 years, it has become more of a crisis than just one of three problems that they have," said Amanda Austin, senior manager of legislative affairs for the business federation. "We basically said, 'We have to be for things, and here's what we're for.' . . . We're just doing what our members want us to do, which is get something."
The insurance industry, meanwhile, could gain or lose depending on which reforms are adopted: Offering tax credits or subsidies to help pay for private coverage for the uninsured could bring insurers millions of new customers; but if a reform law also lets people choose a public Medicare-style plan, private insurers could lose business.
Karen Ignagni, the president of AHIP, which represents insurers covering some 200 million Americans, said her organization began working on a series of reform strategies two full years ago - long before anyone knew who would be president or what the state of the economy would be now - out of a sense of responsibility and pragmatism.
"Strategically, industries have choices if they're at the epicenter of the discussion about a certain part of the economy," she said. "They can sit and wait for others to develop proposals or take the bull by the horns and look at what are the issues that are troubling the country, what are the issues that need to be resolved to help improve the productivity of the country. . . . It's not an altruistic strategy, it's a realistic leadership strategy."
Last month, AHIP announced it would support new regulations prohibiting insurance companies from denying coverage to people with preexisting conditions as long as individuals were required to buy insurance.
The parties still differ on many of the basic elements of any overhaul. Unions and large businesses, for example, oppose changes to the tax exclusion for employer-sponsored coverage - the provision that lets people get health insurance through their employers tax-free - because they fear disrupting the existing system and don't want employees to lose tax benefits. But trimming the tax exclusion for those with higher salaries or more generous benefits could help finance reform for all, specialists say.
AHIP believes that if insurers are required to accept everyone who applies, then individuals should be required to buy insurance. Obama has opposed requiring individuals to buy insurance.
Insurers are also concerned about creation of a public insurance option, something Obama and Senate Finance Committee Chairman Max Baucus have proposed.
Doubtful that the healthcare industry will sacrifice profits for a more efficient and inclusive system, Health Care for America Now, a coalition of mostly left-leaning groups - including MoveOn.org, the massive liberal grassroots organization - is preparing for a multimillion dollar public relations campaign to push through health reform.
"We bring a lot of skepticism to some of the posture that the insurance industry and the small-business community and the drug companies have taken in terms of their professed support for reform," said Richard Kirsch, the national director of the group, which issued a statement challenging AHIP's new proposal yesterday, even before today's announcement.
But Ron Pollack, president of Families USA, a left-leaning healthcare consumer advocacy group, said he believes real progress is quietly being made. He helped organize a 'strange bedfellows' group of 18 organizations - including the Federation of American Hospitals, AHIP and the US Chamber of Commerce - that are meeting regularly with a professional mediator in hopes of reaching common ground on substantive issues.
"If the 'strange bedfellows' participants reach agreement and find common ground, this clearly would be a game-changer," Pollack said. "It would make sure that the contentious atmosphere that pervaded every health reform debate in the past would become a much more cooperative exercise."
---------
"Only health costs keep on climbing"
The Berkshire Eagle - Letters, Tuesday, December 02, 2008
Six years ago, I retired. Each November, I receive notification from my prior employer of any changes to my health insurance contribution for the following year. In 2007, I was notified the contribution would be $200 per month higher than in 2008. I've been notified that for 2008 it will increase another $357 per month. It's become the single largest monthly expense in our household.
When I look at the total cost of medical insurance paid by myself and prior employer, covering me and my wife only, it's over $23,000 per year. Better said, that's $444 per week!
I'm not criticizing my prior employer. What I question is why medical costs and insurance continue to rise at rates that would make the savviest investor drool — in this case, 14.5 percent for 2008 and 22.8 percent for 2009. Wall Street is obviously not the only culprit in the current financial meltdown.
DAVE SIMMONS
Lee, Massachusetts
---------
"Health insurers lay out a path to universal care: Group calls for public-private partnership"
By Lisa Wangsness, Boston Globe Staff, December 4, 2008
WASHINGTON - Leaders of the nation's largest health insurance industry lobbying group yesterday announced a series of proposals they said would help achieve universal coverage, control costs, and improve the quality of care.
"The heart of our proposal is a public-private partnership that builds on the employer-based coverage that 170 million Americans rely on today," said James Roosevelt, Jr., the president and chief executive of Tufts Health Plan. "We have laid out a workable, realistic path to universal coverage. . . . We want to make sure no one falls through the cracks of our healthcare system because of age, health status, or income."
America's Health Insurance Plans, the organization that represents insurance companies covering some 200 million Americans, unveiled the plan at the National Press Club. The proposals - stated so generally that the group's president, Karen Ignagni, said they would be impossible to price - included recommendations for insuring everyone, containing costs, improving quality, and reducing administrative hassles for doctors.
Insurers oppose the creation of a Medicare-style public insurance option, which both President-elect Barack Obama and Senate Finance Committee Chairman Max Baucus have proposed, which they believe will force private companies to compete with the government on an uneven playing field. The insurers also do not support an employer mandate.
The ideas hinge on a proposal the lobbying group put forward last month: Insurers would agree to stop denying coverage to people because of preexisting conditions as long as all individuals were required by law to buy insurance. That would prevent people from buying insurance only when they need it and force younger and healthier people to share the cost of care for older and sicker people.
The insurers also proposed that regulations be revised so that basic high-deductible health insurance plans with a streamlined set of benefits would be available in all 50 states. The "essential benefits" plan would include coverage for wellness and disease management as well as chronic and acute care.
To help make coverage affordable to middle-class people, particularly the self-employed and those who work for small businesses, the government would give refundable tax credits on a sliding scale, according to income. Medicaid should cover everybody under the poverty level, the insurers said, and the State Children's Health Insurance Program should cover all children up to 300 percent of the poverty level.
To help control health costs, the insurers said, Congress should set a goal of reducing the growth of healthcare costs by as much as 30 percent over five years, for a savings of $500 billion, through steps including eliminating unnecessary treatments and paying doctors for better care, not more care.
The insurers' plan also calls for improving the quality of care by devoting more expertise and money to preventive and wellness care; investing in more research to determine the best treatment protocols and providing this information to doctors; and standardizing technology that is used to record and transmit patient information.
Health Care for America Now, a coalition of mostly left-leaning organizations, including the liberal group MoveOn, immediately issued a statement criticizing the insurers, saying their plan would still allow insurance companies to charge older and sicker people huge premiums and would do nothing to cap executive salaries.
But a spokesman for US Senator Edward M. Kennedy, whose staff has been meeting with the insurers and others to develop a reform initiatives, responded positively, saying, "The insurance industry has advanced serious proposals that deserve serious analysis and consideration."
---------
A BOSTON GLOBE EDITORIAL
"Goodbye, Harry and Louise"
December 4, 2008
DURING THE democratic presidential primaries, the key domestic policy disagreement was over the candidates' health reform plans. Should the government require every individual not covered by employers or a public plan to buy health insurance? Hillary Clinton and John Edwards said yes; Barack Obama said no. Now the insurance industry has announced its support for an individual mandate, a move that could bring the country closer to universal healthcare.
Favoring a mandate that everyone must have insurance would seem like a no-brainer for insurers - it guarantees them more customers who can spread the costs around. But the trade group America's Health Insurance Plans and the Blue Cross and Blue Shield Association have added a major concession from their side: In exchange for the mandate they would agree to provide coverage to all comers, whatever their age or preexisting conditions. This could lead to a debate in which insurers are not working to sabotage agreement, as they did with the Harry and Louise ads in the 1990s.
The insurance industry's unwillingness to cover everyone has always been a great hurdle to reform. The industry has resisted any requirement from government that it cover everyone for fear that only the sick would enroll in the new plans, driving up the cost of premiums for all. With an individual mandate, the companies are assured they will also have healthy customers buying policies - because they have to.
The individual mandate is one of the pillars of the Massachusetts health reform law. That law has worked because its designers wisely allowed narrow exemptions for those too rich to qualify for a state-subsidized plan and too poor to buy a commercial one. The designers also came up with a simple enforcement device: Those who fail to buy coverage would be penalized on their tax return. To keep employers from dropping coverage, the Massachusetts law exacts a modest fee from those with more than 10 workers who fail to provide a minimum level of insurance.
The combination of an individual mandate and guaranteed access is also part of the reform plan that the chairman of the Senate Finance Committee, Max Baucus, unveiled last month.
During the primaries, Obama said that his own reform plan, which would mandate insurance for children and lower the cost of it for everyone else, could come close to universal coverage. But Obama should be open to the Massachusetts argument: that an individual mandate with guaranteed access and a mandate on employers would get the country even closer.
There are many hurdles, including rising healthcare costs, ahead. But the Obama administration should seize the opportunity the insurance indusry is presenting, and finally get the nation to yes on universal coverage.
---------
THE BOSTON GLOBE, Op-Ed
LAURA MACCLEERY AND ZACHARY PROULX
"A big pill for healthcare to swallow"
By Laura MacCleery and Zachary Proulx, December 22, 2008
PRESIDENT-ELECT Obama has promised a system of universal healthcare, but enacting one will be far more difficult than it should be. Even with change coming to America, drug companies and other high-spending special interests will keep buying their way onto Capitol Hill if other things don't change first.
The drug companies have mastered the art of purchasing favorable results. In the same election cycle that brought record presidential fund-raising from grassroots donors, the pharmaceutical industry contributed over $22 million to members of Congress. It hedged contributions evenly between the Republican and Democratic parties for the first time in nearly 20 years. Pfizer, a longtime donor to the GOP, is now doling out 51 percent of its campaign contributions to Democratic candidates.
Massachusetts's Department of Public Health has recently proposed regulations to address the influence of drug companies by limiting their payments and gifts to doctors. As critics note, however, the proposal would exempt disclosure of payments to doctors for research and related activities - a stipulation the drug industry lobbied for - which could leave open windows for more foul play.
An investigation launched last year by Republican Senator Charles Grassley of Iowa found government-funded physicians at universities like Harvard and Emory have frequently failed to disclose consulting receipts, stock holdings, and other conflicts-of-interest with drug makers as they research and discuss products. Grassley's investigators found that the former director of the National Institute of Mental Health, Dr. Frederick Goodwin, had failed to disclose at least $1.3 million in income from marketing lectures for drug companies while advocating for their products on his NPR program "The Infinite Mind."
Medical journals have been similarly affected. A British Medical Journal article from 2003 reviewed 30 studies published in journals and found that a "[s]ystematic bias favors products which are made by the company funding the research," and the pharmaceutical company Wyeth was just exposed for paying ghostwriters to publish journal articles.
Whatever shape Massachusetts's regulations take, national healthcare reform has still a bigger pill to swallow, for drug makers also invest, systemically and opportunistically, in politicians. Healthcare PACs do too - they increased donations to Democrats in the latest election cycle by more than 50 percent compared with 2006, according to Congressional Quarterly.
So long as lawmakers need contributions to get reelected, the drug lobby and other special interests will give them, and expect a return on their investment. The only way out of this endless cycle is to dismantle the access-for-favors system and take a different approach to campaign finance.
Public financing of elections would provide a solution, by supplanting private campaign donations with public money and giving lawmakers a shot at legislating beyond the shadow of their donors.
In Maine, for example, state legislators attribute the success of a 2003 healthcare reform effort to public financing. In Arizona, Governor Janet Napolitano, who received public funding for her 2002 and 2006 gubernatorial campaigns, credits public financing with allowing her to offer prescription drug discounts to seniors and the disabled on her first day in office - a program expanded to all Arizonans in 2006.
Just as doctors are courted by drug makers, we have to stop pretending that public officials are immune to the enticements of financial incentives. Our politicians may come to Washington to make change, but they cannot in the current system. Public funding of elections would stop the game of "let's pretend" and allow members of Congress to be both interested in their own political survival and public-spirited.
Kudos to Massachusetts for pursuing what it says will be the strictest law in the country on gifts to doctors and disclosure requirements. Perhaps now it's time we take a page from the pharmaceutical companies' playbook and give elected officials financial incentives that will let them truly serve the public. A public funding system for members of Congress may be the best shot at making real the changes we've been promised.
-
Laura MacCleery is deputy director of the Democracy Program at the Brennan Center for Justice at NYU School of Law. Zachary Proulx is a research associate at the Brennan Center.
-

-
---------
"A look at hospital troubles across the country"
By The Associated Press, December 27, 2008
Hospitals around the country are struggling to stay afloat amid the recession, although many have had financial problems for years, often blamed on Medicare, Medicaid and other government health programs that don't fully cover the costs of care for millions of patients.
Some recent developments:
--In mid-December, the prestigious Cleveland Clinic started a hiring and salary freeze across the 33,000-worker health system; it also restricted travel and use of consultants and contractors.
--In New Jersey, five of the 79 acute care hospitals in business at the start of 2008 have closed, most recently Muhlenberg Regional Medical Center, and a sixth may close soon. In early December, the state health department said it would dole out $44 million to six others to keep them from closing or slashing services.
--Other recent hospital closures include the 617-bed Physicians Medical Center Carraway in Birmingham, Ala.; Century City Doctors Hospital in Los Angeles, and Lincoln Park Hospital, in an upscale Chicago neighborhood.
--The Healthcare Association of Hawaii in November reported hospitals there posted their eighth straight year of losses and said the situation will worsen. The two-hospital Hawaii Medical Center filed for bankruptcy, several hospitals have laid off large numbers of workers and the Hawaii Health Systems network of about a dozen public hospitals needed a $13 million advance in late August to avoid shutting down.
--Numerous hospitals have filed for bankruptcy, including Charlotte, N.C.-based Hospital Partners of America, which operates four hospitals; Michael Reese Medical Center in Chicago and Associated Healthcare Systems Inc., which has four rural hospitals in the South; and North Oakland Medical Centers in Pontiac, Mich.
--Many hospitals are laying off workers, trimming the hours of part-timers and reducing use of more-expensive temporary nurses hired through agencies. Among them are the four-hospital St. Vincent's Health System in Alabama; Boston Medical Center, which primarily serves immigrants and poor people, and the Columbia St. Mary's system, which has four hospitals in Milwaukee and Mequon, Wis.
--Nashville-based HCA Inc., the nation's No. 1 private hospital chain with about 160 hospitals, is cutting about 110 jobs and closing most functions -- even the emergency department -- at its Portland, Tenn., hospital, and laying off roughly 100 headquarters staffers.
-- For-profit Tenet Healthcare Corp., which operates 56 hospitals in 12 states, has seen patient volumes dip, missed Wall Street expectations in the third quarter and warned it may not make its financial targets next year. Its shares have been hammered, plunging from $6.55 in early September to $1.10 by Christmas.
--Some hospitals have been posting multimillion-dollar losses or had credit rating agencies put their bonds on credit watch or downgrade their ratings. Some investor-owned hospital companies have seen share prices plummet, missed Wall Street forecasts or lowered their own financial performance predictions. Along with trimming expenses and delaying capital projects, some are discussing mergers or selling medical office buildings to raise cash.
---------
"Generic drugs slow health care spending"
By Kevin Freking, Associated Press, Tuesday, January 06, 2009
WASHINGTON — Spending on health care slowed slightly in 2007 as consumers turned more to generic drugs instead of brand-names to fill their medicine cabinets, the government reported Monday.
Although the cost of buying drugs, visiting the doctor or going to the hospital continued to increase faster than the overall economy, the 6.1 percent growth rate for all health care spending was the slowest since 1998. In 2006, spending increased 6.7 percent.
Officials worry that devoting more and more resources to health care makes it harder for families to meet other pressing priorities and for businesses to compete internationally.
Overall, Americans spent $2.2 trillion on health care, an average of $7,421 a person, for the year.
About 67 percent of medications dispensed in 2007 were generic drugs — up from 63 percent the year before. Generics can cost as little as one-third the price of brand-names.
Several factors are helping to drive the increased use of generics. First, insurers are steering consumers to lower-priced medicines by charging low co-payments for certain drugs. Meanwhile, they charge higher co-payments for medicines they want consumers to avoid for safety and financial reasons.
Large retailers and grocers are encouraging consumers to buy generics by enticing them into their stores with low prices.
Several blockbuster brand-name drugs lost their patent exclusivity in 2006, generating competition. Notable examples include Flonase, an allergy medicine; Zocor, a medicine used to lower cholesterol; and Zoloft, which is used to treat depression.
Federal officials said safety concerns also probably influenced spending on medicine. The Food and Drug Administration issued more of its most serious warnings than in previous years — 68 in 2007 versus 58 the year before and 21 in 2003.
Another aspect of the overall spending slowdown came from a decrease in administrative expenses associated with the new Medicare drug benefit. The program kicked in during 2006, generating a substantial uptick in administrative expenses.
Officials emphasized that the good news about slowing the increasing costs of health care extended only to prescription drugs. All other major health sectors — such as hospitals, physicians, nursing homes and home health — grew at the same rate or slightly faster than the year before.
Since prescription drugs generate only about 10 percent of all health spending, officials question how much longer the transition to generics would dampen the growth in health care costs.
"I wouldn't expect the good news to continue," said Richard Foster, chief actuary for the Centers for Medicare and Medicaid Services.
Historically, health spending has been somewhat insulated from the effects of a slowing economy, which means health care makes up an even greater share of the overall economy during recessions. In 2007, the health sector's share came to 16.2 percent, up from 16 percent the year before.
Among the major components of the health industry, officials found:
Hospital spending, which makes up nearly one-third of all health spending, increased 7.3 percent. In the 1990s, spending on hospital services grew at a 5.2 percent rate, thanks in part to more tightly managed care from insurers.
Spending for physicians and clinical services grew 6.5 percent, the same rate as the year before.
The cost of nursing home care increased 4.8 percent.
Spending for home health care increased by 11.3 percent.
Spending for private health insurance grew 6 percent, unchanged from the year before but much lower than in 2002 when it hit 10.7 percent.
The entire report appears in the journal Health Affairs.
---------
"The fight for health reform"
The Berkshire Eagle, Editorial, Saturday, January 10, 2009
While President-elect Barack Obama is to be praised for attempting to usher in an era of good feeling after far too many years of ugly, paralyzing partisanship in Washington, there are programs that will have to be fought hard for in the months and years ahead. One of them is health care reform, and the battle lines are already being drawn.
Tom Daschle said all the right things Thursday in a hearing before a Senate committee on health that is sure to lead to his confirmation as head of the Department of Health and Human Services. Contrasting the Obama administration's approach to health care reform with that of President Clinton, who left Congress out of the picture to his ultimate regret, the former South Dakota senator and majority leader promised to involve Congress at every stage. He said the administration's three main goals would be to provide health insurance for all Americans, lower the costs of insurance, and place a greater emphasis on prevention, all admirable aims. The challenge, however, is in making them reality.
Senator Mike Enzi of Wyoming, the ranking Republican on the health committee, says his party wants any new coverage offered to uninsured Americans to come through private insurance plans, but it is the private insurers who are at the root of many of the system's long-standing problems. The president-elect wants to expand public health programs, an important component of reform that Republicans will oppose, based on early indications.
There will always be partisanship in a two-party system, and debate and dissension are healthy, but ending the divisive partisanship of the past eight years is necessary, and it will take two parties to end it. Democrats must work with Republicans, while advocating for their platform. The Republican Party has its agenda too, but should it ignore the will of Americans expressed at the ballot box, it will be inviting its third straight defeat at the polls.
---------
The Boston Globe, Op-Ed, CLAUDIA MEININGER GOLD
"Medication can't fix a broken childhood"
By Claudia Meininger Gold, January 26, 2009
ON ONE recent day in my pediatric practice, I saw or spoke with parents of eight children who had experienced a range of significant trauma. One was in foster care after living on the streets with drug-abusing parents. Some had been adopted following severe abuse and neglect. One had recently lost a parent to death, one had been abandoned by a parent. They were failing in school, impulsive, distracted, angry, and depressed. They were receiving minimal to no mental health support.
What they all had in common was a diagnosis of attention deficit hyperactivity disorder. Each parent expected that I would either: refill the medication, change the medication, change the dose of medication, or have the medication given at a different time.
When I suggested that medication alone was not the solution, I ran into walls. One mother had tried to get an appointment with a child psychiatrist, but the only one in town who accepted her insurance wasn't taking any new patients. My attempts to refer families for therapy were thwarted by many things, including lack of time and clinicians who did not take their insurance. One parent was irate that I asked so many questions and didn't just refill the prescription. These parents were discouraged and angry, and by the end of the day, so was I.
Our society has bought into a belief that manipulating medications will fix these complex problems. Not only parents, but teachers, physicians, and certainly the health insurance and pharmaceutical industries join in promoting this expectation. With our overreliance on psychoactive medication, we have created another Ponzi scheme where, just as Bernard Madoff's investment fund was not really earning any money, we are fooling ourselves into thinking that we are helping these children in any significant way.
For hope, and possible answers, I turn to another visit in my practice. A mother of a 4-year-old had struggled with her daughter's intense, inflexible temperament. She had felt embarrassed and alone. She and her husband had fought terribly under the strain of sleep deprivation and the challenge of parenting this difficult child.
But they had gotten help. In couples therapy they had learned to join together in their efforts to help their daughter manage her strong feelings. In telling me her story, this mother recognized how her own life experiences may have affected her ability to accept her daughter as the person she is. In the mother's relationship with me, she has felt accepted and fully supported, and has been able to do the same for her daughter. In the years I have known this family, I have watched this child grow to be a bright, engaging little girl, who is now thriving in preschool.
So what does this story have to offer? Being an effective parent, even under the best of circumstances, is the most difficult job there is. In their efforts to help their daughter, these parents found multiple supportive relationships - with each other, with their therapist, and with me. All the latest research integrating developmental psychology, genetics, and neuroscience shows that secure early relationships between parents and children lead to the development of capacity for emotional stability, flexibility, and sociability. Put simply, children need their parents. So if we are going to nurture our children, we must first and foremost nurture their parents.
The parents of the children with attention deficit hyperactivity disorder that I spoke with that day have no such support. They are on their own to manage these troubled children. It is understandable that they turn to a pill, for there are few other options. As is clear from the story of my 4-year-old patient, meaningful help for parents comes through relationships. Primary care doctors, who develop relationships over time, can be an invaluable source of help to parents. High quality, accessible mental health services can also provide this kind of relationship.
But our current healthcare system places preventive primary care and mental health care at the bottom, when they should be of highest value. Once we have a system in place to truly support these parents, we will enable them to help their children in meaningful and long-lasting ways.
-
Claudia Meininger Gold is a pediatrician in Great Barrington, Massachusetts.
-
---------
"Falling through health care cracks"
The Berkshire Eagle, Letters, Thursday, January 29, 2009
Our country's health care plan will only cover people if they have the money to do so. It's either your money, or you die. In the United States, about 47 million people are uninsured and about 22,000 of these people die every year because of their lack of health coverage. The uninsured in our country do not have health insurance because they either can't afford their employer's health coverage plan or cannot afford to buy their own. Some employers don't even offer health insurance to their employees. About three-quarters of uninsured adults are not eligible for public health care plans, such as Medicaid.
Our country should be searching for a way to get health coverage for all citizens. The uninsured are 4.5 times more likely to not receive medical care simply because they cannot afford it and are also more likely to develop disabilities over time due to lack of medical services. In fact, the uninsured are likely to spend about 2.5 times more on services than it would cost an insured person if they had to pay in full. This is because the United States does not have a fixed cost for medical services or prescriptions. If the United States could find a way to get fixed prices on these medical services like countries such as Canada, then the uninsured would have less of a blow to take.
Although such plans as Medicaid and Medicare try to alleviate the amount of uninsured Americans, our country loses up to $130 billion a year due to the lack of productivity lost from uninsured Americans unable to work.
Medicare covers senior citizens above the age of 65 as well as younger Americans with permanent disabilities, while Medicaid offers health coverage for those who make very low income. However, this does not lower the amount of uninsured Americans that are able to work and cannot due to lack of medical coverage. Our country needs to form a way of gaining money through taxes or some other source in which an overall health care plan would be funded.
KURTIS KEEFNER
Great Barrington, Massachusetts
---------
"At Wal-Mart, a Health-Care Turnaround: Once Criticized, Company Is Now an Innovator in Employee Coverage"
By Ceci Connolly, Washington Post Staff Writer, Friday, February 13, 2009; A01
Washington policymakers contemplating a fundamental overhaul of the nation's troubled health-care system may want to study the saga of Wal-Mart.
Once vilified for its stingy health benefits, the world's largest company has become an unlikely leader in the effort to provide affordable care without bankrupting employers, their workers or taxpayers in the process. From its headquarters in Bentonville, Ark., the retailer is doing in the real world what many in Washington are only beginning to talk about.
At a time when other firms are scaling back or eliminating health coverage, Wal-Mart has made a serious dent in the problem of the uninsured. New figures being released today show that 5.5 percent of its employees now lack health insurance, compared with a nationwide rate of 18 percent.
The company has also put into practice many of the innovations that experts say will lead to higher-quality, more efficient care. Using its high-tech marketing savvy, Wal-Mart has introduced digital records, partnered with prestigious organizations such as the Mayo Clinic, and begun targeting costly health problems such as obesity and premature births.
Yet for all of Wal-Mart's achievements, the story of its immersion in the world of health policy is also a warning about the depth and breadth of one of the thorniest challenges facing the country today.
In attempting to strike a balance between healthy profits and healthy workers, Wal-Mart, like many businesses, still falls short of the comprehensive care that President Obama says he wants for Americans.
To reach near-universal coverage, the largest private employer in the nation relies heavily on the government and other employers to play a role. Of the company's 1.4 million workers, 52 percent are in a Wal-Mart health plan. Despite revenue that is expected to exceed $400 billion for 2008, the company charges its low-wage workers a substantial portion of their income for medical coverage.
Though proud of what it sees as dramatic progress, Wal-Mart itself warns that in a global market with a weakened economy, it cannot -- or will not be able to -- accept annual health-care increases of about 8 percent indefinitely.
"It starts to impact us competitively," said Linda Dillman, the company vice president tapped to oversee the health plan.
To Andrew Stern, president of the Service Employees International Union and a frequent Wal-Mart critic, the company's health contributions are not commensurate with its financial success. The moral, he said, is that "volunteerism has its limits."
But to Mark Smith, head of the California HealthCare Foundation, an independent nonprofit focused on health-care quality and efficiency, Wal-Mart's experience provides a different lesson.
"Even a company as big and successful as Wal-Mart cannot possibly solve this problem on its own," he said. "There are limits to what one company can do."
'It Had to Do Something'
It began with an internal memo, union agitators and some awfully bad press.
In fall 2005, the union-sponsored Wal-Mart Watch got its hands on a company memo outlining ways to clamp down on soaring health-care bills. Among the suggestions: Stop hiring unhealthy people.
Frustration with Wal-Mart had been building. Main Streets across the country chafed at the big-box store's arrival; labor activists complained that workers had to wait up to two years to qualify for the company health plan, which in many cases cost nearly 10 percent of the typical $20,000-a-year salary.
Yes, some U.S. companies did not provide any health insurance. But the skimpy Wal-Mart coverage seemed particularly galling compared with the billions in personal wealth amassed by the company's founding family, the Waltons.
The retailer symbolized by a bright-yellow smiley face was suddenly tagged with a red bull's-eye. Unions underwrote two aggressive anti-Wal-Mart campaigns, staffed primarily with Democratic political operatives. Teachers boycotted the back-to-school shopping season.
Several states, including Maryland, considered legislation in 2006 requiring that large employers commit a certain portion of their revenue to employee health care. Though the bills never said so, they were aimed at just one company.
The criticism stung, but more important, it began to affect the bottom line. Between 2000 and late 2005, Wal-Mart's stock fell 27 percent.
"It was hurting them when they tried to open a new store," Smith said. "For normal competitive reasons and its corporate image, it had to do something."
In 2006, then-chief executive Lee Scott appointed Dillman, his technology guru at the time, to take over health care. Though she maintains that Wal-Mart's program was never as bad as opponents suggested, Dillman moved quickly to make changes.
First, the wait to enroll in the health plan was reduced from two years to one for part-time employees and to six months for full-time workers. By the following year, an additional 50,000 workers were eligible.
Next, Wal-Mart put its marketing genius to work, doing sophisticated research on its own personnel.
"Any retailer will tell you that's what they do with their customers," Dillman said in a recent interview. "There are very sophisticated methods of doing this. If you want people to sign up, go find out what they need."
Employees said they wanted more choices, especially low-cost emergency coverage options. Wal-Mart responded with a menu of deductibles, co-payments and maximum out-of-pocket costs. It teamed up with the Internet site WebMD to simplify enrollment, created electronic health records and expanded its $4 generic drug plan from the 350 medications available to customers to more than 2,000 for employees.
Many workers have chosen low-premium, high-deductible plans that analysts say provide less coverage for preventive and primary care. The company tries to mitigate that with an upfront credit of between $100 and $500 that can be used on any medical expense.
"We're seeing utilization on types of care you would hope," such as checkups and the generic drugs, Dillman said. "And they're managing costs at the same time."
From 2007 to 2008, the retailer saw a 78 percent increase in 16-to-24-year-old workers who opted for the high-deductible plans. "It's better to have them in that than to have nothing, which is where most of them were," Dillman said.
Others, such as Cynthia Murray of Hyattsville, say a $180 premium out of a biweekly paycheck that averages $489 after taxes is too steep. Murray and her husband have been without health coverage for the nine years she has worked at Wal-Mart. "I just pray a whole lot I don't get sick," she said.
Seeking the Best Value
At the opposite end of the spectrum, Wal-Mart contracted with the Mayo Clinic for all transplant services, calculating that it could save money by using a single provider with a sterling performance record.
Whether purchasing toasters or transplants, "Wal-Mart looks for value," said Brooks Edwards, director of Mayo's transplant center in Rochester, Minn., one of several Mayo centers around the nation. "One of the most cost-effective things we do is weed out the patients that don't need a transplant."
Where other medical centers might recommend a heart transplant, for example, Mayo might opt for a simpler valve surgery. The strategy of evaluating various treatments, known as comparative effectiveness research, is gaining currency in policy circles. The economic stimulus bill sets aside $1 billion to pursue it.
Wal-Mart's newest initiative, "Life With Baby," is aimed at reducing the rate of premature births among employees, which is double the national average, Dillman said. Mothers-to-be are matched with a registered nurse who counsels them on issues such as diet, stress and smoking. The support continues with lactation instruction and vaccinations for the child's first year.
"Wow, it was really good. It helped me so much," said Cristina Majano, a 23-year-old new mother who works at a Wal-Mart in Northern Virginia.
For her first four years on the job, Majano did not purchase health insurance. "I was younger and didn't think I needed it," she said.
The coverage, even with a $1,000 deductible, is worth it for her and her daughter, Majano said. But she and her husband decided they could not afford to add him to the plan.
Wal-Mart, taking a cue from leading policy analysts, hopes to continue to focus on major cost drivers, moving next to back pain and diabetes.
"This is like the national discussion," Dillman said. "First you've got to get them in the plan, then figure out how to help them take care of themselves, stay healthy and get the care they need."
-
Research editor Lucy Shackelford contributed to this report.
-
Employee Health Coverage: More than half of Wal-Mart employees get their health insurance through Wal-Mart, a percentage that has increased after the company lowered the waiting period for eligibility and expanded deductible choices.

-
---------
PHYLLIS GREENBERGER, Op-Ed, The Boston Globe
"Why one size doesn't fit all in medicine"
By Phyllis Greenberger, February 23, 2009
SEX matters - especially in the doctor's office.
Many prescription drugs, including antihistamines, antidepressants, and heart medications, work much differently on men and women. Women are also more vulnerable to certain diseases. Eighty percent of those with osteoporosis are women. Heart disease kills over 50,000 more women than men each year. And women are more than twice as likely to suffer from depression.
The difference between the sexes is worth keeping in mind as the Obama administration implements its plan for a Federal Coordinating Council for Comparative Effectiveness Research. Created as part of the economic stimulus package that was signed last week, the council stands a good chance of improving the quality of healthcare delivery nationwide by codifying best practices and developing world-class clinical guidelines for medical treatments.
Witness the success of Premier Inc., a national alliance of thousands of hospitals and healthcare sites.
By collecting data from its members, Premier is able to analyze which treatments, practices, and techniques yield the best results. This information is stored in a database accessible to participating physicians, administrators, and other healthcare personnel, helping them make more informed decisions.
By harnessing the extraordinary resources of the federal government, the newly created council could similarly improve the delivery of care.
There is a risk, though. Elsewhere in the world, comparative effectiveness research has been used to ration treatments. Such research has also gained a reputation for a one-size-fits-all approach to medicine.
In Britain, the National Institute for Health and Clinical Excellence has been issuing appraisals of medical treatments for close to a decade. The institute considers both cost effectiveness, which measures the benefits of a treatment against the expense to provide it, and clinical effectiveness, which measures how much better a newer treatment is for patients than an older one. The agency then makes recommendations to Britain's National Health Service about which treatments are worth covering.
Sometimes, though, the agency's findings prevent people from getting the best care possible. Last year, for instance, the institute recommended that the National Health Service not cover the life-extending lung cancer drug Tarceva because of its price tag. Even though the institute's decision was eventually overturned, some British cancer patients were denied their last hope for staying alive.
As the American comparative effectiveness agency is assembled in the coming months, administrators must take into account the personal needs of individual patients. If the council were to primarily focus on cost effectiveness, it would likely only consider the "average" patient. But in medicine, every patient is unique.
Just consider all the differences between men and women. At every level of the human body - the system, organ, tissue, cellular, and sub-cellular - there are a host of differences between sexes. Only recently have we started to understand how these differences impact the prevention, diagnosis, and treatment of disease. This underscores why physicians must have the freedom to prescribe the treatments best suited to the particular patient for whom they're caring.
The law does ensure that "subpopulations are considered when research is conducted," but this is hardly a guarantee that comparative effectiveness research won't one day be abused at the expense of patients in the United States.
Lawmakers had the right idea when they created the council. It's now up to the Obama administration and the Department of Health and Human Services to make sure that this new body is used properly.
Otherwise, doctors could find themselves unable to provide individual patients with the personalized treatments they need. That would leave all of us - men and women alike - worse off.
-
Phyllis Greenberger is president and CEO of the Society for Women's Health Research.
-
Source: www.boston.com/bostonglobe/editorial_opinion/oped/articles/2009/02/23/why_one_size_doesnt_fit_all_in_medicine/
-
---------
"Health care costs to top $8,000 per person"
By Ricardo Alonso-Zaldivar, Associated Press Writer, February 24, 2009
WASHINGTON --A new government report on medical costs paints a stark picture for President Barack Obama, who is expected to call for a health care overhaul in a speech Tuesday night to a joint session of Congress.
Even before lawmakers start debating how care is delivered to the American people, the report shows the economy is making the job of reform harder.
Health care costs will top $8,000 per person this year, consuming an ever-bigger slice of a shrinking economic pie, says the report by the Department of Health and Human Services, due out Tuesday.
As the recession cuts into tax receipts, Medicare's giant hospital trust fund is running out of cash more rapidly, and could become insolvent as early as 2016, the report said. That's three years sooner than previously forecast.
At the same time, the government's already large share of the nation's health care bill will keep growing.
Programs such as Medicaid are expanding to take up some of the slack as more people lose job-based coverage. And baby boomers will soon start reaching 65 and signing up for Medicare. Those trends together mean that taxpayers will be responsible for more than half of the nation's health care bill by 2016 -- just seven years from now.
"The outlook for health spending during these difficult economic times is laden with formidable challenges," said the report by statisticians at HHS. It appears in the journal Health Affairs.
The health care cost forecast did not take into account recent legislation that expanded medical coverage for children of low income working parents, and added to the government's obligations.
The report "accelerates the day of reckoning," said economist John Palmer of the Maxwell School at Syracuse University.
"It is bringing home more immediately the problematic dimensions of what we face," added Palmer, who has served as a trustee overseeing Social Security and Medicare finances. "The picture was bad enough ten years from now, but the fact that everything is accelerating gives greater impetus to be concerned about health reform."
The report found health care costs will average $8,160 this year for every man, woman and child, an increase of $356 per person from last year.
Meanwhile, the number of uninsured has risen to about 48 million, according to a new estimate by the Kaiser Family Foundation.
The government statisticians estimated that health costs will reach $13,100 per person in 2018, accounting for $1 out of every $5 spent in the economy.
Policy makers would like to slow the rate of increase in spending, but that has proven difficult, because American-style medicine care relies on intensive use of costly high-tech tests and procedures.
In a separate report, also due out Tuesday, private researchers looked at spending on medical conditions and found that the most costly were mental disorders -- including Alzheimer's -- and heart problems.
The White House says Obama believes that out-of-control costs are the main obstacle to securing coverage for all.
"Health care costs are crushing middle class families and the small businesses that fuel job growth in this country," said White House spokesman Reid Cherlin. "President Obama believes that if we're going to get our economy back on track, we have to act quickly to address this pressing issue."
-
On the Net: www.healthaffairs.org
-
---------
"Budget would reserve $634b for healthcare: Obama signals he will work with Congress"
By Ceci Connolly, Washington Post, February 26, 2009
WASHINGTON - President Obama intends to release a budget today that would create a 10-year, $634 billion reserve fund as a down payment on a vast expansion of the US healthcare system, an overhaul expected to cost as much as $1 trillion over the next decade.
Obama would pay for the expansion by trimming tax breaks for the wealthy and tightening payments to insurers, hospitals, and physicians, according to a senior administration official.
By first identifying a large pot of money to underwrite a healthcare overhaul reform - before laying out a proposal on who would be covered or how - Obama hopes to signal his willingness to negotiate with Congress over the details of an eventual plan.
"We wanted to get this process going by putting some serious resources on the table," said the official, who was not permitted to speak publicly until formal release of the budget blueprint. "This is a reserve fund instead of a 700-page plan. We learned the lessons of the past and want to work interactively with Congress. This is a first step."
Yesterday, Douglas Elmendorf, head of the Congressional Budget Office, told the Senate Finance Committee that without changes in policy, the number of uninsured Americans will rise from 45 million to about 54 million over the next decade.
Under the Obama budget blueprint, about half of the new "healthcare reserve fund" would come by limiting the tax break on itemized deductions for families with incomes above $250,000. The proposal would reduce the value of tax deductions by about 20 percent, a change which would generate about $318 billion over the next 10 years, according to administration documents provided to The Washington Post.
Throughout the campaign, Obama promised to reduce the number of uninsured Americans, improve the quality of care, and save the typical American family $2,500 a year in medical costs. He has remained firm to his pledge to press ahead this year.
The budget "includes a historic commitment to comprehensive healthcare reform - a down payment on the principle that we must have quality, affordable healthcare for every American," the president said in his address to Congress Tuesday night. "It's a step we must take if we hope to bring down our deficit in years to come."
Many of the itemized savings are both familiar and controversial to segments of the health industry.
Nearly one-third of the reserve fund would be generated by forcing private insurers who sell Medicare managed care plans to undergo a competitive bidding process. Currently, the government pays the plans, known as Medicare Advantage, about 14 percent more than traditional fee-for-service Medicare coverage, according to estimates by the Congressional Budget Office.
Drug manufacturers and hospitals would face reductions as well. If the budget is approved, drug companies would be required to increase the rebate they now provide for medications sold to Medicaid patients from 15 percent to 21 percent. The proposal will probably spark a ferocious lobbying campaign by the industry, which has argued that the current 15 percent rebate is already cutting into profits.
The budget figures also represent significant shifts in how the United States will pay for medical care in the future.
For example, specialists have identified hospital readmissions - especially for elderly patients - as a sign of inadequate care and unnecessary expense. About 18 percent of Medicare patients are readmitted to the hospital within 30 days of their original visit. The new approach would establish flat fees for the first hospitalization and 30-day follow-up. Hospitals with high readmission rates would be paid less.
According to the Associated Press, Obama's proposed budget also proposes a mix of tax cuts for the middle class and tax increases for upper-income households. That includes extending beyond 2010 the $400 annual tax cut in the stimulus plan just signed into law.
The budget also calls for an increase in the top income tax rate, from 35 percent to 39.6 percent for couples with incomes above $250,000 a year, an administration official said. It would also freeze the estate tax at current levels rather than allowing it to permanently expire next year, the AP reported.
The biggest tax adjustment, however, would come from updating the alternative minimum tax for inflation.
---------
A BOSTON GLOBE EDITORIAL
"The court rules for patients"
March 6, 2009
WHEN THE Supreme Court upheld a $6.7 million award Wednesday to a Vermont woman who lost an arm in a botched drug injection, the verdict went against not just the drug maker but also the Food and Drug Administration. The drug company, Wyeth, argued that the FDA's approval of the injection method and label warnings about its risks immunized the company against lawsuits in state courts. But the judges were only too aware of the FDA's long history of failure to keep unsafe drugs off the market.
The 6-to-3 ruling sends two messages. It tells President Obama that he can waste no time fulfilling his pledge to strengthen the FDA. Justice John Paul Stevens's opinion for the majority specifically refers to the agency's limited resources.
Second, the ruling tells the pharmaceutical industry that it bears final responsibility for the way its products are made and administered. It cannot hide behind the approval of an FDA that has shown a weakness for approving drugs before they are sufficiently tested and then failing to monitor closely the drugs' often harmful side effects once they are on the market.
At issue in Wednesday's ruling was not the drug itself, the anti-nausea medication Phenergan, but the warning on its label for how it should be administered. Diana Levine lost an arm to gangrene after a clinic worker mistakenly injected the drug into an artery. Injection into a vein is one of three methods of administering the drug. After successfully suing the clinic, Levine's lawyer also persuaded a Vermont jury that Wyeth's label on the drug should have carried a much stronger warning against the injection method. Stevens pointed out that, prior to Levine's treatment, there had been 20 other cases in which injections of Phenergan had led to gangrene and amputation.
Wyeth said it should not be found liable because the FDA had approved the label warning. The court rejected that view, stating that the law and FDA regulations make it clear "that the manufacturer bears responsibility for the content of its label at all times." The decision echoes another case in which the court did not let industry use federal law as a shield: the December ruling that consumers can sue tobacco companies over the marketing of "light" cigarettes.
Critics of the court's Levine decision worry that it will cause pharmaceutical companies to steer away from innovative drugs in favor of modest improvements to existing medications. It need not have that effect, however, if companies would test their new medications more thoroughly before bringing them to market, and then do a better job of monitoring adverse events and reacting to them decisively.
---------
"Just laid off? Go for COBRA"
Posted by Cheryl Costa, boston.com, March 5, 2009
The new stimulus law contains several great breaks for taxpayers. One in particular really helps those who have recently lost their jobs and are wondering how they are going to afford health insurance. Previously in this blog, we have written about the importance of continuing health care coverage when you lose your job. In most instances, the best option is to continue health coverage under the Consolidated Budget Reconciliation Act of 1985 (COBRA). Now, the COBRA option is even more attractive.
Starting March 1, 2009, anyone who loses their job between August 31, 2008 and December 31, 2009 can elect coverage under COBRA and 65% of their premium will be paid by the government for up to nine months. That's a huge savings considering the cost of coverage for a family can be $1,000 per month or more. For example, without this new break, a family would be responsible for paying the full monthly COBRA premium. Now, the family would pay only 35 percent or $350 per month. Over nine months, that is a total savings of almost $6,000.
To be eligible for the subsidy, you must have been "involuntarily terminated". And, if you left your job before February 17, 2009 and you declined coverage, you must be given a 60 day window to elect coverage. Be on the lookout for a notice from your previous employer advising you of the opportunity to re-elect coverage.
It is important to note that there is no income limit for taking advantage of this subsidy. However, if you do take advantage of this option, the amount of the subsidy will be considered taxable income if your 2009 adjusted gross income (AGI) exceeds $125,000 for single taxpayers and $250,000 for married couples filing jointly.
---------
"Wal-Mart to enter electronic medical records arena"
By Associated Press, Wednesday, March 11, 2009, www.bostonherald.com, Healthcare
WASHINGTON — As the Obama administration begins investing billions in health information technology, Wal-Mart plans to use its unrivaled size to bring high-tech medical records to U.S. physicians.
In recent years Wal-Mart, the world’s largest retailer, has used its buying power to move into health care markets, negotiating steep discounts for prescription drugs and eye care products.
With the government providing $17 billion of stimulus funding to encourage use of electronic medical records, the company sees an opportunity to serve as a low-cost, one-stop option for single doctors and small practices.
A Wal-Mart spokesperson said Wednesday the company is partnering with computer giant Dell Inc. and software maker eClinicalWorks to launch a bundled electronic health records package for doctors, including installation and maintenance.
The program will be offered through the company’s Sam’s Club discount-warehouse division, which caters to small businesses. A formal launch is expected this spring.
"Because of our volume, our size and our relationships we can leverage what we do for our members every day into this service," said spokesperson Susan Koehler, in a telephone interview from the company’s Bentonville, Ark., headquarters.
Improving the nation’s health information technology has been a rallying cry in Washington for years. Advocates say replacing paper files could reduce costly medical errors and duplicative testing. But after nearly a decade of promotion, there have been few gains to show for the technology.
Less than 20 percent of the U.S. physicians use electronic medical records, and many complain about the upfront costs of going digital and the daunting technological hurdles for small businesses.
Consulting group Avalere Health said this week it would cost about $124,000 for a single doctor to upgrade to electronic health records over five years.
Wal-Mart believes it could shave somewhere between 30 and 50 percent off that figure, putting the price closer to $44,000, the maximum in incentive payments available to single-practice physicians.
"We will streamline the process and be a single point of contact for them," Koehler said
Under the plan, Dell will provide computers and other hardware while eClinicalWorks will provide and install the software. Wal-Mart’s role will be to coordinate the process.
The Obama stimulus package will pay out $17 billion in incentives beginning in fiscal 2011 to spur adoption of electronic medical records by doctors and hospitals. Those payments will gradually taper off through 2015 and then become penalties for those not using the technology.
Investor’s expectations for the plan have lifted shares of companies like Cerner Corp., the leader in hospital-installed electronic records, in recent months. Other companies poised to benefit include McKesson Eclipsys Corp. and Allscripts-Misys Healthcare Solutions Inc.
-
Article URL: www.bostonherald.com/business/healthcare/view.bg?articleid=1157912
-
---------
"Dean talks health reform: Former governor speaks in Berkshire County at Dowmel Lecture Series"
By Trevor Jones, Berkshire Eagle Staff, Thursday, March 12, 2009
GREAT BARRINGTON — After spending four years helping Democrats regain control of Congress and the White House, former Vermont Gov. Howard Dean, says he ready take on his next big challenge — health care reform.
Dean, who was governor from 1995-2003 and then served the last four as head of the Democratic National Committee, spoke Wednesday night at the Dowmel Lecture Series at Monument Mountain High School.
He said health care reform in the coming years is achievable.
President Obama's plan will be more approachable to Americans, according to Dean, because it contains options that already exist to many.
"You have to appeal to the American people, and I like Barack Obama's health care plan, not because it's perfect, but because it could be easily explained to people," said Dean.
Dean said the president's plan would allow people to elect to keep their current insurance or take federal insurance already in place — Medicare.
Dean said he believes reform can happen this time because nearly all the necessary parties are behind it.
While he expects Republicans and insurance companies to oppose the measure, he said it will be at their own peril.
"If (Republicans) want to filibuster and kill health insurance reform, they will be a smaller party than they are today and we'll get it passed in 2011," said Dean.
And while reforms to the current system are essential, according to Dean, the most important long-term goal is to improve the way Americans look at their personal health care.
"We have to be willing to change to a system that is based on a wellness model, and not an illness model," said Dean.
Meeting with reporters before the event, Dean spoke about his future in politics, the president's job performance and what his career as a politician and as a physician have in common.
"There's lots of ways to be involved in politics. You don't have to just be appointed or elected to office to do that," said Dean, who declined to comment on recent rumors about potential positions in the Obama administration.
He did say the President Obama has done a great job so far, giving him an "A-plus" for his work and saying people are wrong to accuse him of taking on too much at once.
"The people who try to attack (Obama's administration) don't realize how inter-related these things are," said Dean.
And on his two career's similarities: "They are both — if done right — both helping professions."
Dean was the final speaker of the series' season, which will return in the fall for the 15th and final season.
Next season's speeches will begin in October, and include Arthur Levitt, Zalmay Khalilzad, Roland Fryer, Mark Hertsgaard, Neil deGrasse Tyson and Bill Moyers.
---------
A BOSTON GLOBE EDITORIAL
"Next stop, health reform"
March 15, 2009
PRESIDENT OBAMA gets high marks for courage and vision in pushing for health reform during the worst economic downturn since the Depression. The challenge will be to get Congress to approve thoroughgoing revisions to the system in the face of special interests that will decry them as threats to both jobs and profits. Change you can believe in is easy; health reform you can believe in will be a tall order.
Still, in less than two months of his presidency, Obama has already changed the health landscape in significant ways. He signed the expansion of the State Children's Health Insurance Program, which will add 4 million youngsters to the 7 million it now covers. His stimulus package includes $20 billion for electronic medical records and $1.1 billion for research comparing the effectiveness of different treatments. Both tools are crucial for sweating waste out of the system.
Most significantly, his 10-year budget includes $634 billion in new revenues and savings as a down payment on the cost of covering the 47 million Americans - and rising - who are now uninsured.
This is all sound groundwork. For the next stage of real changes in the system, Obama has drawn a lesson from the behind-closed-doors Clinton health reform debacle of the 1990s: Congress, the drug industry, medical device makers, insurers, doctors, and hospitals must be involved in basic decision-making. This is wise, but only if Obama and congressional leaders make clear that none of these interests gets a veto over the broad outline for reform that Obama laid down as a candidate.
.
Lessons from the Clinton years
This will doubtless be a sticking point with insurers, who dread having to compete with Obama's proposed new, Medicare-like public insurer for consumers younger than 65. Candidate Obama's health plan was less fully developed than John Edwards's or Hillary Clinton's. But by backing a public alternative, Obama showed he understood the necessity of an affordable option for those who cannot get work-based insurance, either because their employer does not offer it or because they aren't working.
The need for such a public provider - and yardstick - is vividly evident in Time magazine's March 5 cover story. Reporter Karen Tumulty recounts in heartrending detail her time-consuming effort to get an insurer in Texas to pay for treatments for her brother, who suffers from kidney disease.
Health reform in the United States has stalled in the past not just because of missteps by elected officials like Bill Clinton but also because most of the 250 million who have insurance are more or less satisfied with their coverage - and are worried about how change in Washington might limit their options or raise their costs. Tumulty points out that many of the 250 million insured are actually underinsured, just one serious disease or injury away from financial ruin. She cites the 2005 finding of Harvard's Elizabeth Warren: that half of all bankrupties in the United States are caused by medical bills and, in 75 percent of those cases, the people filing for bankruptcy actually had health insurance.
.
The Massachusetts example
The Clinton experience from 1993 to 1994 offers "how not to" tips on healthcare reform. Massachusetts, whose 2006 reform plan now covers almost 98 percent of residents, can provide some "how to" tips. One is that Congress should assemble strong majorities in both houses for its health bill. The Massachusetts plan won the support of a Republican governor, a Democratic Legislature, advocates for the poor and underserved, and representatives of business, hospitals, the insurance industry, and healthcare professionals. This consensus has helped the program weather a need for increased funding from all sides last year.
The chairman of the Senate Finance Committee, Max Baucus, told the Globe recently that he hopes his committee's health bill will win the support of 75 of the 100 senators. This would provide it far more than the 60 votes needed to stop a filibuster by opponents. But there have been reports out of Washington that reform advocates might try to push through a bill as part of a budget reconciliation measure, which cannot be filibustered and thus could pass with as few as 51 votes. This could be a mistake.
In Massachusetts, reform won such broad support in part because the bill focused solely on expanding access to the uninsured and did not attempt to control health cost inflation at the same time. This could work in a relatively rich state, in which healthcare and medical research are seen as economic mainstays. But evading the difficult choices that cost-cutting requires is not an option for Congress.
The escalating cost of care is at least as pressing a problem as the scandal of the uninsured. The nation's healthcare system consumes one-sixth of the Gross Domestic Product, but the World Health Organization in 2000 ranked it just 37th in the world for quality. France, which spends 51 percent per capita what the United States does, was first.
Obama has got it right. Fixing healthcare cannot wait until the economy is back on its feet because its waste, inefficiencies, and special-interest coziness are a drag on economic growth. Skyrocketing health costs for workers and retirees are a key cause for Detroit's collapse. Indeed, all US firms seeking to compete internationally carry the albatross of bloated health costs.
Ratcheting back the nation's medical bills while also extending coverage in a way that commands a solid congressional majority is a daunting task. But the price of inaction is steep: constantly spiraling cost increases for a healthcare system that does not even cover all Americans.
----------
-

-
Patrick Tumulty with his medication and his bills. (Dan Winters for TIME)
-
"The Health-Care Crisis Hits Home"
By Karen Tumulty, San Antonio, TIME, Thursday, March 05, 2009
When you've been strong and fit your whole life, it can be easy to discount your body's first whispers of sickness as merely the side effects of daily living. Looking back over the past three years, my older brother Patrick now understands the meaning of his increasingly frequent bouts of fatigue, his fluctuating appetite and the fact that his blood pressure had crept up to 150/90. But Pat had always put off going to the doctor until he had to. Having bought health insurance that carried a $2,500 deductible, he knew he would have to pay for a checkup himself. That is no small consideration for someone who makes $9 an hour, as my brother did in his job as an administrative assistant for a lighting firm in San Antonio. He also struggles with Asperger's syndrome, a disorder sometimes described as high-functioning autism. Pat can multiply three-digit numbers in his head with ease, but he has trouble accepting the unfamiliar and adjusting to the unforeseen.
The unforeseen was exactly what turned up when Pat went in for a physical on Nov. 30, 2007, his first in five years. The doctor found high levels of blood and protein in his urine, results that were confirmed in another round of tests in December. Soon after that, Pat discovered that his urine had turned brown and foamy. In the middle of all this, he was laid off from his job, and finding a new one while doing temp work was his most pressing concern. Finally, last July my brother's doctor insisted that he see a specialist, who quickly ordered a biopsy. That's when Pat, who is now 54, learned that his kidneys were failing.
The diagnosis was only the first shock. The second came a few weeks later, in an Aug. 5 letter from Pat's health-insurance company. For six years — since losing the last job he had that provided medical coverage — Pat had been faithfully paying premiums to Assurant Health, buying a series of six-month medical policies, one after the other, always hoping he would soon find a job that would include health coverage. Until that happened, "unexpected illnesses and accidents happen every day, and the resulting medical bills can be disastrous," Assurant's website warned. "Safeguard your financial future with Short Term Medical temporary insurance. It provides the peace of mind and health care access you need at a price you can afford."
Kidney failure would seem to be one of those disastrous "unexpected illnesses" that Pat thought he was insuring himself against. But apparently he was wrong. When my mother, panicked, called to tell me that the insurance company was refusing to pay Pat's claims, I told her not to worry; bureaucratic mix-up, I assumed. I said I'd take care of it, bringing to bear my 15 years of experience covering health policy, sitting through endless congressional hearings on the subject and even moderating a presidential candidates' forum on the issue.
Confident of my abilities to sort this out or at least find the right person to fix the problem, I made some calls to the company. I got nowhere. That's when I realized that the national crisis I'd written so much about had just hit home.
The previous four weeks had left my brother with more than $14,000 in bills from hospitals, doctors and labs. And that was just to figure out what was wrong with him. Actually treating his disease was going to be unimaginably more expensive. Patrick needed help quickly, and we didn't have a clue where or how to start looking for it.
.
The Underinsured
When we talk about health-care reform, we usually start with the problem of the roughly 45 million (and rising) uninsured Americans who have no health coverage at all. But Pat represents the shadow problem facing an additional 25 million people who spend more than 10% of their income on out-of-pocket medical costs. They are the underinsured, who may be all the more vulnerable because, until a health catastrophe hits, they're often blind to the danger they're in. In a 2005 Harvard University study of more than 1,700 bankruptcies across the country, researchers found that medical problems were behind half of them — and three-quarters of those bankrupt people actually had health insurance. As Elizabeth Warren, a Harvard Law professor who helped conduct the study, wrote in the Washington Post, "Nobody's safe ... A comfortable middle-class lifestyle? Good education? Decent job? No safeguards there. Most of the medically bankrupt were middle-class homeowners who had been to college and had responsible jobs — until illness struck."
If there is a ground zero for both problems, it is Texas, where I grew up and where my parents and brothers still live. About 1 in 4 Texans is uninsured, the highest rate in the country. The vast majority of the uninsured — 8 in 10 — live in households in which someone works, typically for a small business. But only 37% of Texas companies with fewer than 50 employees offer medical coverage.
The state's Medicaid program is notoriously stingy. State law requires counties to provide care only to those deemed "indigent," defined as people who earn less than 21% of the federal poverty line, or $2,274 a year for a single adult and $4,630 for a family of four. Many counties, particularly rural ones, do no more than that minimum. So Texas — a state with relatively little regulation of the health-insurance industry — is fertile territory for insurance companies selling bare-bones coverage at low prices.
But falling ill without adequate insurance leaves you at risk no matter where you live. Since 2005, the American Cancer Society (ACS) has maintained a national call center for cancer patients struggling with their bills. In that time, more than 21,000 people have called in asking for help. Every story is different, but the contours of the problem tend to be depressingly similar: the 10-year-old leukemia patient in Ohio who, after three rounds of chemotherapy and a bone-marrow transplant, had almost exhausted the maximum $1.5 million lifetime benefit allowed under her father's employer-provided plan; the Connecticut grocery-store worker who put off the radiation treatments for her Stage 2 breast cancer because she had used up her company plan's $20,000 annual maximum and was $18,000 in debt; the New Hampshire accountant who, unable to work during his treatment for Stage 3B stomach cancer, had to stop paying his mortgage to afford a $1,120 monthly premium for coverage with the state's high-risk insurance pool.
What makes these cases terrifying, in addition to heartbreaking, is that they reveal the hard truth about this country's health-care system: just about anyone could be one bad diagnosis away from financial ruin. Most people get their coverage where they work. But Anna McCourt, a supervisor at the ACS call center, says employees often have difficulty understanding the jargon in insurance policies. Even human-resources personnel may not fully understand all the intricacies of a policy when briefing a new employee. Coverage that seems generous when you are healthy — eight annual doctor visits or three radiation courses — quickly proves insufficient if you find yourself really sick.
.
Between Coverage and Safety Net
Pat's decision to save some money by buying short-term insurance was a big mistake, says Karen Pollitz, project director of Georgetown University's Health Policy Institute and a leading expert on the individual-insurance market. "These short-term policies are a joke," she says. "Nobody should ever buy them. It is false security that is being sold. It's junk."
That's because diagnosing and treating an illness may not fall neatly into six-month increments. While Pat had been continuously covered since 2002 by the same company, Assurant Health, each successive policy treated him as a brand-new customer. In looking back over Pat's medical records, the company noticed test results from December, eight months earlier. Though Pat's doctors didn't determine the precise cause of the problem until the following July, his kidney disease was nonetheless judged a "pre-existing condition" — meaning his insurance wouldn't cover it, since he was now under a different six-month policy from the one he had when he got those first tests.
After 33 years of wrestling with insurance companies, Deborah Haile, payment coordinator at the San Antonio Kidney Disease Center, where Pat went for treatment, has pretty much figured out the system. So when I put in my first desperate call to her, on Aug. 20, 2008, she offered to make another run at Assurant. Within an hour, Haile called back, her voice bristling with anger. "Cancel that policy," she advised me. "Your brother is wasting his money on premiums, and he's going to need it."
There was at least one thing we didn't have to worry about, Haile assured me. Pat's kidney doctor, Peter Smolens, would keep treating him even if he couldn't pay. Smolens, a thin, soft-spoken man, later told me that about 10% of his patients have inadequate insurance or none at all. He has agonized with some as they struggled with hard choices, like whether to have a hospital biopsy or pay their mortgage. As a physician, he said, "you just see them. You know you're not going to get paid."
As grateful as we were for Smolens' forbearance, that still left us with the question of how to keep up with the rapidly mounting bills for drugs and lab work. Haile put us in touch with B.J. Smith, a social worker at the center. Patient and reassuring, Smith turned out to be the angel we needed. She had only recently returned to work after taking off seven years to stay home with her two children. The first thing she advised Pat was to start paying his bills, all of them, even if it meant putting down only a few dollars a month on each one. Otherwise, everything he had — his one-bedroom condominium, 2003 Saturn Ion and $36,000 in savings — would be put at risk, as the letters from collection agencies had begun to arrive. Smith called Pat's medical creditors one by one and set up the arrangements: $51.89 a month to one hospital, $76 to another, installments of $4.78 a month to $111.89 a month on six different sets of LabCorp bills. Then there was the $626 he owed two radiologists. One agreed to knock off $22 as a hardship discount, writing Pat, "We are happy that we could be of assistance to you and your family in this time of need."
A paradox of medical costs is that people who can least afford them — the uninsured — end up being charged the most. Insurance companies, with large numbers of customers, have the financial muscle to negotiate low rates from health-care providers; individuals do not. Whereas insured patients would have been charged about $900 by the hospital that performed Pat's biopsy (and pay only a small fraction of that out of their own pocket), Pat's bill was $7,756. For lab work — and there was a lot of it — he was being charged as much as six times the price an insurance company would pay. One pathology lab's bill alone was $3,290.
Over time, with Smith's guidance, Pat learned to trim his bills here and there. Instead of refilling small prescriptions, for instance, he could buy some drugs more cheaply in bulk. (A hundred pills of one blood-pressure medication was less than $16 at Costco, compared with $200 at the pharmacy.) But that didn't address the cost of his care going forward. Pat's kidney function, which was 48% when Smolens first saw him last summer, has fallen to between 35% and 40%. And there are now outward, obvious signs of Pat's illness: he is lethargic, his eyes are puffy, and his lower legs and ankles are swollen to twice their normal size.
The disease — whose cause Pat's doctors doubt they will ever know — is winning. Now Smolens is trying to figure out whether Pat, whose Asperger's gives him a low tolerance for the demands of a complicated medical regimen, should move from his current medications to a more aggressive approach that includes immuno suppressing chemotherapy drugs. The newer drugs can cost $10,000 a treatment; even the old ones can easily run $500 a month. "It's almost like a black hole in terms of the potential costs," Smolens told me. "But when you look at the alternative — progressive kidney failure — then you're talking about having to receive dialysis, and the average cost of dialysis treatments in this country is $60,000 per year plus."
There's another paradox: if Pat gets sick enough to need dialysis, as he well may, the Federal Government will pick up those staggering costs under the Medicare program for end-stage renal disease. But until that point is reached — and the goal is to keep him from getting there — his options are limited. Now that he is sick, it would be nearly impossible for him to purchase another insurance policy on the individual market. Since he lives independently and holds a job, it would be difficult for him to qualify for Social Security disability benefits. While Texas, like 34 other states, has a high-risk pool for those who are hard to insure, the program is twice as expensive as an average individual health-insurance policy. And my brother would have to wait 12 months to join with a pre- existing condition, under the state's "adverse selection" regulations that seek to prevent uninsured people from joining the pool only after they get sick.
As we were running out of options, Smith told us there was one more avenue to try. Bexar County — where San Antonio is located and an estimated 30% of people under 65 do not have health coverage — has a health-care program for the uninsured that is far more generous than most in Texas and practically unique in the country. Rather than continuing to wait for the uninsured to show up in its emergency rooms, in 1997 the Bexar County hospital district established a system called CareLink for those who make 200% of the poverty line or less. (In his current job, answering queries that come in to a text- message information service, Pat earns $1,257 a month, which means he qualifies.)
CareLink operates much like a health-maintenance organization for its 55,000 clients, negotiating prices with health-care providers and then billing clients on a sliding scale according to their income. (Pat's CareLink bills run around $40 a month.) And it puts a heavy emphasis on preventive care; on Pat's first examination at an austere CareLink clinic in northwestern San Antonio, he got tetanus and flu shots as part of the deal. Another stroke of good fortune: Pat's kidney doctor, Smolens, is a participating specialist with CareLink.
For primary care, CareLink assigned Pat to Dr. Carolyn Eaton, an engaging woman who has been working with the system for about a year. What alarms her most about the new patients she has seen lately, Eaton says, is how long people wait — diabetics whose feet are numb, cancer patients already in the advanced stages of the disease — before they seek treatment. "When people fall on hard times, they're kind of embarrassed," Eaton says. "Their health care ends up becoming much more expensive."
It's not a seamless system. Pat gets confused navigating between Smolens, who prescribes tests and medications, and CareLink, which must approve them. "The fact is, for guys like Pat, it requires a lot more work to do the same sorts of things" that would be a snap if he had insurance, says Smolens, sighing.
.
The Limits of Personal Choice
As this country prepares to engage in its first serious debate over comprehensive health-care reform in 15 years, there are two leading approaches to covering the 45 million uninsured and reining in costs. One, which President Barack Obama is putting forward, would force more employers to offer coverage to their workers, with subsidies and other incentives to make it more affordable. The other, advocated by Republicans (including Senator John McCain in the recent presidential campaign), would take away some of the tax advantages that come with getting coverage at work and thereby put many Americans who are now covered by their employers into the marketplace on their own. The idea is that they would be the ones best equipped to decide which plan suits their individual needs.
Pat's experience suggests it is difficult for an individual to make such judgments. And the existing market for these kinds of policies leaves a lot to be desired. A 2006 Commonwealth Fund study found that only 1 in 10 people who shopped for insurance in the individual market ended up buying a policy. Most of the others couldn't find the coverage they needed at a price they could afford.
The individual health-care consumer has very little power or information. Still, it turns out that there are ways to fight back. As I was reporting my brother's story, I discovered something about Pat's former insurance company: last May, insurance regulators in Connecticut imposed a record $2.1 million in penalties on two Assurant subsidiaries for allegedly engaging unfairly in a practice called postclaims underwriting — combing through short-term policyholders' medical records to find pretexts to deny their claims or rescind their policies. In one case, a woman whose non-Hodgkin's lymphoma was diagnosed in 2005 was denied coverage because she had told her doctor on a previous visit that she was feeling tired. Assurant agreed to pay the fine but admitted no wrongdoing.
So I contacted the Texas Department of Insurance, identifying myself as both the sister of an aggrieved policyholder and a journalist. Officials there suggested that Pat file a complaint against the company. Each year the department receives as many as 11,000 complaints and manages to get $12 million to $13 million back for consumers, Audrey Selden, the department's consumer-protection chief, told me. "It is important to complain."
And it's easy too. It took Pat and me less than 10 minutes to fill out the complaint form over the Internet. That was Jan. 14, 2009. On Feb. 9, we had an answer: Assurant maintained that it had done nothing wrong and that Pat should never have relied on short-term coverage over a long period. But given "the extraordinary circumstances involved," the company agreed to pay his claims from last year, when the policy was still in force. (Pat canceled it on Aug. 22, 2008.) Those extraordinary circumstances, I assume, included the fact that the state insurance department was sniffing around.
After we received the insurance company's decision, I tried to talk to Assurant for this story. Its only response was a written statement from Scott Krienke, senior vice president for product lines: "Due to privacy regulations, we cannot discuss the specifics of any of our customers' coverage." But he also noted that "Assurant Health's Short Term Medical product is designed for people experiencing a break in the continuity of their permanent medical coverage. Our Individual Medical plans are more appropriate for those who have an ongoing need for medical coverage."
I wish the company had told my brother that when it sold him the policy in the first place.
-
Related News Article Link: www.time.com/time/nation/article/0,8599,1883149-1,00.html
-
---------
"Defining ‘Health Care Reform’"
By Uwe E. Reinhardt - Uwe E. Reinhardt is an economics professor at Princeton.
The New York Times - economix.blogs.nytimes.com, Economix: Explaining the Science of Everyday Life - Today's Economist, March 27, 2009
In his news conference Tuesday night, President Obama stated that he was willing to be flexible on negotiating with Congress on the budget for the 2010 fiscal year, but that he would stand firmly by his commitment to “health care reform.” It sets off the question of what he and others mean by that term.
Here is a brief explanation of what he’s probably referring to.
As a horizontal economist lying in a hospital bed, I, like most patients, tend to think of health care as a caring human activity in which I repose my trust.
As a vertical economist, however, I naturally think of health care as just another economic sector with the following distinct facets:
1. a demand side (by which I mean patients or their agents, private and public health insurers, who procure health care and pay for that care)
2. a supply side (the providers of health care and of health care products)
3. a health-insurance system, intended to protect individuals and households from excessive financial loss due to medical bills, and also to help patients procure health care at negotiated prices
4. an information infrastructure supporting and linking patients, insurers and providers of care with one another, and
5. a regulatory infrastructure intended to keep transactions in this market honorable, fair to both sides, and oriented toward the ultimate social goals of a health system.
Ambitious as he is, the president would like to reform all of these facets of the health sector.
First, on the demand side, he would like to move the United States closer to the almost-century-old goal of attaining universal health-insurance coverage. The idea is to endow with adequate purchasing power the rapidly growing number of low-income Americans who cannot afford to pay for health care of a satisfactory quality. I shall explain in a next post what all that entails, especially how much it might cost in added public spending.
Next, also on the demand side, the president would like to reform the manner by which we pay the providers of health care. The general idea is to align payments with actual “performance” through what is now known as “pay-for-performance” or simply P4P. Ideally such a system would be based on so-called “bundled payments” for an entire medical case treated in accordance with evidence-based clinical practice guidelines.
Although an old idea, it has eluded implementation so far, because it is horrendously difficult to achieve in practice. For a taste of how difficult it is, the reader may wish to view this and this.
The ultimate objective of this demand-side policy, however, is to goad the supply side through financial incentives into delivering genuinely clinically integrated health care, in place of the traditionally fragmented care they now deliver. It would require a major realignment of professional and economic power on the supply side.
Third, on the health insurance facet, the president would like to develop a well-functioning market for individually purchased health insurance, as an alternative to the employment-based system which covers most insured non-elderly Americans.
There now is such a market, but it covers only a small fraction of non-elderly Americans, primarily because it is highly fragmented and, moreover, in most states pegs the individual’s insurance premiums to that individual’s health status. To reform this market, the president would establish a National Insurance Exchange.
This can be thought of as the analogue to a farmers’ market on which competing insurers offer their products, subject to a set of regulations that make transactions in the market transparent and honorable, and the competition among insurers fair.
A major contentious issue here is whether the insurers competing in this market should include a newly established public insurance plan like Medicare, but for the non-elderly.
Fourth, on the information facet supporting both sides of the market, the president and Congress jointly already have earmarked close to $50 billion for the development of an electronic health-information infrastructure.
That infrastructure would contain an electronic medical record, through which clinicians anywhere in the health system can have access to an individual patient’s medical record, intended to safeguards of the patient’s right to privacy.
Over the longer run, there would also be a so-called personal electronic health record that links individual patients electronically to their medical record and to their primary care physicians.
Such an information infrastructure would make available, to patients and other users, information on the quality of health care rendered by individual providers of health care — e.g., hospitals and physicians. This access would facilitate better cost- and quality-control emanating from the demand side of the system.
It would also disseminate information from what should be called “cost-effectiveness analysis,” but, as was discussed in earlier posts, has been constrained to be mere “comparative effectiveness analysis” (see this and this for more on this subject).
Finally, to make all of these pieces work harmoniously together — toward the social goals of improving the health status of Americans by providing all of them with access to timely care, and of protecting their budgets from undue inroads of medical bills — there would have to be a whole set of additional government regulations, mainly on the health insurance industry.
This is a challenging set of tasks, some of which warrant further discussion. I plan to trigger it with some subsequent posts.
---------
"Intel, GE to spend $250 million on health products"
The Associated Press, Thursday, April 2, 2009
NEW YORK (AP) — Intel and General Electric are jointly investing $250 million over the next five years to develop products aimed at providing personalized home health care technology for seniors.
The companies envision technology that will cut health care costs and help aging baby boomers and people with chronic illnesses remain in their homes by allowing doctors to monitor patients remotely.
Announcing the agreement today, Intel Corp. Chief Executive Paul Otellini and GE CEO Jeffrey Immelt said their cooperation will help them jump quickly into a market they estimate will grow to $7.7 billion by 2012, from $3 billion this year.
The investment is one of "four or five big bets" that Intel, the computer chip maker, is making outside of PCs.
---------
"Report: NE states fall short on tobacco prevention"
boston.com - April 13, 2009
BOSTON --Health advocates say New England states have failed to deliver on a pledge to use money from the tobacco settlement for prevention programs, with most states funding programs at only 20 percent of recommended levels.
The Campaign for Tobacco-Free Kids released a report Monday, saying Connecticut, Massachusetts, New Hampshire, and Rhode Island are funding tobacco prevention programs at less than 20 percent of the Center for Disease Control's recommendations.
The report also says Maine and Vermont are the only New England states funding tobacco prevention at half the CDC's recommended levels.
Officials say New England states will spend only 2.3 percent of the $1.8 billion in tobacco settlement and tax revenue on tobacco prevention programs this year.
---------
"Diabetics skimp on lifesaving care in recession"
By Linda A. Johnson, Associated Press, Monday, April 13, 2009
Diabetics are increasingly risking life and limb by cutting back on — or even going without — doctor visits, insulin, medicines and blood-sugar testing as they lose income and health insurance in the recession, an Associated Press analysis has found.
Doctors have seen a drop in regular appointments with diabetic patients, if they come back at all. Patients more often seek tax-subsidized or charity care. And they end up in emergency rooms more often, patients and physicians said in interviews.
Sales of top-selling drugs and other products used to treat and monitor the disease have dropped since the economic crisis accelerated last fall, the AP analysis found. There are even signs that some patients are choosing less-expensive insulin injections over pricier pills to save money.
Meanwhile, the number of people with the disease keeps growing — another 1.6 million Americans were diagnosed in 2007 alone.
People with other health problems also are cutting back on care amid the recession, but diabetics who don't closely monitor and control the chronic disease risk particularly dire complications: amputations, vision loss, stroke — even death.
Patients' frugality comes at a tremendous cost to the already-strained health care system. The typical monthly bill to treat diabetes runs $350 to $900 for those without insurance, a price tag that's risen as newer, more expensive medicines have hit the market. Emergency care and a short hospitalization can easily top $10,000, and long-term complications can cost far more.
M. Eileen Collins, 48, of Indianapolis, tried to scrimp on her medication last fall after her husband lost his job and with it their insurance. Without money for insulin, test supplies and other medicines, she asked for free samples and also got a few drugs through $4-a-month generic programs. But she stopped taking most of her drugs and cut her insulin doses in half to stretch her budget.
'I was just real careful'
"I truly did not think I was putting my life in danger," Collins said. "I thought if I was just real careful with what I ate ... I'd be all right."
By Thanksgiving eve, Collins was vomiting blood and rushed to a hospital. Doctors diagnosed her as malnourished, anemic and in diabetic ketoacidosis, a life-threatening condition caused by lack of insulin and sky-high blood sugar. She spent a week in the hospital.
Her story is hardly unique.
Dr. Steven Edelman, a University of California, San Diego endocrinologist who runs a free clinic staffed by medical students, has seen a 30 percent surge the past six months in patients seeking free diabetes medicines and supplies, which the clinic has to ration. Many had been solidly middle class, but the recession took their jobs, insurance and even some homes.
"A third to a half of these people haven't been taking their meds at all," said Edelman, who also founded the advocacy group Taking Control of Your Diabetes.
Diabetes occurs when the body doesn't make enough insulin or doesn't efficiently use the hormone, which helps turn sugar from food into energy. The disease can be kept under control by monitoring blood sugar as well as exercising, improved diet, medications, testing and regular checkups.
Sales of diabetes testing supplies and drugs indicate how many Americans have moved beyond scrimping and are cutting vital expenses. Several doctors said they began noticing a shift in August or September, when the financial markets melted down and layoffs accelerated.
Sales have dipped for pricey brand-name diabetes pills, blood glucose monitors and even test strips, based on industry sales figures and interviews with the top two makers of testing supplies. The strips generally cost $1 or more each; patients using insulin are supposed to test at least two to four times a day to be sure their blood sugar is in a safe range.
Sales of the most widely used pill, $4-a-month metformin, are up 7 percent since June, according to the AP analysis of figures from health data firm IMS Health Inc. Brand-name versions of the same drug, costing 10 times as much, are down 9 percent, on average, since then.
Diabetes cases on the rise
By February, sales for nearly every other category of diabetes pills and insulins were down from a year earlier, most by double digits, IMS figures show. The only exceptions were a heavily promoted new type of diabetes pill, Januvia, and advanced insulins that tightly control blood sugar levels.
The sales declines come even as the number of diabetes cases grows, fueled by the rise in obesity. According to the American Diabetes Association, more than 24 million Americans have diabetes.
Emergency rooms increasingly are treating diabetics who haven't been taking medicines, according to doctors at several hospitals nationwide and the professional group for ER doctors.
Many of the patients have blood sugar so high they are hospitalized for days. Free clinics also are getting a surge of diabetes patients desperate for help.
"There's an increase in just overall consequences of diabetes: losing a foot, losing a kidney, bad eyesight. At least six people come to mind over the last six months ... most because of the recession," said Dr. Nicholas Vasquez, who works in one of the country's biggest ERs, at St. Joseph's Hospital in Phoenix.
"What we're seeing mostly is the first steps of people not taking care of their diabetes and starting to have consequences," he said.
---------
"In North Carolina, Recession Breeds a Health-Care Crisis: Job Losses Leave State With Highest Percentage of Uninsured"
By Ceci Connolly, Washington Post Staff Writer, Monday, April 20, 2009
GREENSBORO, N.C. -- It's right there on the wall, hectoring David Talbot as he races from one exam room to another.
"You want to see the recession? There it is," Talbot says, pointing to a row of multicolored graphs. "We began to spike in October 2008, and we're losing the battle now. We just can't keep up."
Recessions are tallied in numbers -- jobless claims, home foreclosures, plant closings and bailout dollars. Here at the HealthServe community clinic, Talbot, the medical director, tracks the recession in days -- the number of days that patients wait to see a doctor.
Just six months ago, the clinic delivered same-day care to most callers, the gold standard from a health perspective. But in October the delays crept to four days, then 19 in November and 25 in December. In January, HealthServe temporarily stopped accepting new patients, and almost immediately 380 people put their names on a waiting list for when the crunch eases.
In North Carolina, more than any other state, the recession has triggered a burgeoning medical crisis. A steep rise in unemployment has fueled a commensurate increase in the number of people who do not have health insurance, including many middle-income families.
"I used to be upper middle class," said Amy, who called HealthServe every morning for weeks before getting in to see Talbot. "I've paid my taxes for 30 years."
Last fall, when she moved here from Florida to care for her parents, she got trapped in the economic tailspin. The former resort manager who bought jewelry in tony Palm Beach now does temp work and sits in the clinic's crowded waiting room with dozens of others who cannot afford insurance.
"I haven't told anyone I'm coming here," she said, asking that her last name be withheld because she is embarrassed to be seeking discounted medical care.
Though in relatively good health, Amy, 54, needs a doctor to monitor her allergies and high cholesterol. "It's kind of depressing," she said. "But thank God it's here."
In the past two years, North Carolina's number of uninsured has climbed 22.5 percent, the biggest jump in the nation, according to an analysis by the North Carolina Institute of Medicine, a quasi-state agency. Nationwide, about 22 percent of adults do not have health insurance. Here in North Carolina, 25 percent of adults -- or 1.8 million people -- have no coverage. An additional 9 percent are underinsured.
For most Americans, health insurance and employment are linked. Every 1 percent increase in the jobless rate translates into 1.1 million people losing coverage nationally, according to the independent Kaiser Family Foundation. North Carolina's unemployment rate has doubled in the past year to 10.7 percent, making it the fourth-highest in the country.
"Relative to other states, North Carolina is still a manufacturing state," said North Carolina State University economist Michael Walden. "And manufacturing takes it on the chin during a recession."
The downturn has hit the state's textile industry, auto-parts factories and real estate businesses. Charlotte, the nation's second-largest financial hub, has seen layoffs. Drugmakers in the Research Triangle are scaling back, and so is Dell Computer.
Unsure where to turn, many patients head to the nearest hospital, said R. Timothy Rice, president and chief executive of the nonprofit Moses Cone Health System. Emergency room traffic there has risen 3.6 percent in the past six months. That increase, coupled with the surging demand at HealthServe, which the system runs, has prompted Rice to open another clinic just a mile away.
The clinics cost Moses Cone between $1.5 million and $2 million a year, but they are cheaper than treating those patients in the emergency department, Rice said.
"I can lose some money in one place or lose a lot more in the other," he said. And at the clinics, social workers and pharmacists provide additional services that patients do not get in the ER.
At Piedmont Health Services in central North Carolina, chief executive Brian Toomey measures the recession in job applicants. Until the economic meltdown, health professionals had their choice of good jobs. Many changed often for higher pay and benefits.
A year ago, Toomey scrambled to fill 40 openings. Now there are five. When Piedmont recently advertised for a part-time dentist, he received 10 résumés. "It's just unheard of" in the normally recession-proof industry, he said.
With revenue down and the number of uninsured patients up, Toomey had been poised to trim the staff. But an infusion of $680,000 in federal economic recovery aid means he can retain 10 to 15 positions.
In all, North Carolina community health centers have received $11.2 million in stimulus money, said Mary Wakefield, head of the U.S. Health Resources and Services Administration.
The clinics are lifelines for people such as Becky Pattishall who do not qualify for Medicaid but have been buffeted by the economic squalls.
Last month, her full-time job as a dental hygienist in Durham was cut to two days a week and her health insurance disappeared. At age 62, private coverage is exorbitant, and her 401(k) "has tanked."
Pattishall's boyfriend, a 49-year-old computer technician who has had blood clots in his lungs, was laid off in the fall. Keeping his health insurance is a top priority.
"We just didn't see this coming," Pattishall said. "I've gone back on my anti-anxiety medication."
North Carolina's hospitals, which have received no stimulus money, count the recession in dollars lost.
The sprawling University of North Carolina Health Care System provided $215 million in free care in the fiscal year that ended last June, said chief executive William Roper. This year, the nonprofit hospital network is on track to deliver $270 million in "uncompensated care."
It's not just the uninsured who are adding pressure to the system, Roper said. Even the insured are reluctant to come in for profit-generating "optional" procedures such as eye surgery or knee replacement because of fears about the eventual impact of the bad economy.
"Our paying customers are slowing down, and our nonpaying customers are surging to unprecedented numbers," he said. "We're getting hit in both directions."
At the HealthServe clinic, Talbot's team has whittled the waiting list to about 180. But that number troubles him, too. Decades of experience tell him that many people will fall through the cracks, discouraged by the long waits, unable to get transportation to the clinic or overwhelmed by the succession of woes that accompany an unemployment rate near 11 percent.
"The problems just cascade. It's that last little blow to the household income that puts them in crisis," he said. "And the scary thing for them is they know if they lose their insurance now, there's a good chance they'll never get it back."
-

-
---------
The Boston Globe, Op-Ed, ROBERT KUTTNER
"Facing down the private insurance industry"
By Robert Kuttner, June 4, 2009
DESPITE BUDGET pressures, President Obama has not backed off his commitment to universal healthcare reform. But the devil is in the details. And if he is not careful he could end up with a reform worse than nothing.
A crucial question is whether the law will include a public, Medicare-style plan. This public plan could be used by people who otherwise lack good insurance, or by employers who conclude that the public plan is a better deal for themselves and their workers.
The public plan would be the gold standard of both good coverage and cost-containment. Without the public option, a system to cover everyone by relying on the existing private insurance industry will realize few cost savings. The result would be increased pressures over time to cut care and shift out-of-pocket costs from insurers to consumers.
The administration's projections have relied heavily on the supposed savings of better use of computerized medical records. However, absent a single unified system, or a strong public option, better computerization will not realize major savings.
The US healthcare system is the most expensive and least cost-effective in the advanced world mainly because private insurance companies waste about 25 cents on the dollar on claims, profits, administration, and marketing. They have no serious financial incentives to emphasize prevention, and every possible incentive to avoid sick people. Doctors and hospitals, meanwhile, make their money from increasing costs.
Other countries get better results at lower cost because a universal system naturally emphasizes wellness and prevention, and spends its money on the most cost-effective treatments, not the most expensive ones. Every nation faces similar inflationary pressures because of advances in technology and an aging population; but other advanced countries, using single-payer systems, do a fine job of covering everyone for 10 percent of gross domestic product or less, while we spend upwards of 15 percent and leave out nearly 50 million souls and under-insure tens of millions more.
Obama's plan is a variant of an astute strategy first proposed by the political scientist Jacob Hacker as a solution to two political obstacles to health reform. First, how do you enlist the uninsured and the anxious insured in the same coalition? Second, how do you build momentum for a single-payer system recognizing that there are not the votes to legislate it all at once?
Hacker's insight was that if the government offered a public insurance option, people who liked their present private insurance could keep it, while others could elect the public plan. Coalition problem solved. And the superior efficiencies of the public plan would gradually overtake the rival private plans. Momentum problem solved.
But Hacker neglected one key political detail - the immense power of the private insurance industry. Not surprisingly, the industry's stance is that any public plan must compete on disadvantageous terms. And most Republicans oppose a public plan outright.
Obama, the great conciliator, has chosen to work with the private insurance industry rather than targeting it as the primary obstacle to meaningful health reform. Periodic leaks from the White House suggest that if push came to shove, Obama would ditch the public plan in order to get a bill through Congress.
Senator Max Baucus of Montana, chair of the Senate Finance Committee, is no enthusiast of a public plan. After the New York Times last week reported Baucus sparring with Senator Ted Kennedy on whether to include a public plan, the two senators quickly cobbled together a statement insisting they were really in harmony.
However, in the push to get legislation in the face of fierce industry and Republican opposition, a good public plan could well be tossed overboard. That would leave a legacy of expanded coverage, but a time bomb of exploding costs, underinsurance, and a squeeze on actual care.
I would much rather see Obama battling for public health insurance, making it clear to Americans that the obstacle to real reform is the private health insurance industry. That, however, is not the president we have.
We'll see what kind of public plan, if any, survives.
-
Robert Kuttner is co-editor of The American Prospect and a senior fellow at Demos. His recent book is "Obama's Challenge."
-
---------
-
www.time.com/time/politics/article/0,8599,1885032,00.html?xid=rss-topstories
-
---------
-
www.boston.com/news/local/massachusetts/articles/2009/06/07/voters_gather_across_us_to_hold_discussions_on_healthcare/
-
---------
A BOSTON GLOBE EDITORIAL
"Calculating insurance interests"
June 25, 2009
LAST WEEK, three insurance executives made starkly clear why President Obama is right to insist on a public-plan option in any health reform package. The three stood before Congress and refused to stop the practice of canceling coverage of sick policyholders for unrelated medical reasons, even in cases where the firms can’t show intentional fraud by the policyholders. The industry should be relieved that all Obama is threatening it with is a rival plan and not a SWAT team.
The industry’s bloodless term for pulling the coverage of patients with non-group policies even after they have paid years of premiums is “rescission.’’ Companies rescind policies - and save themselves millions in pending claims - even when there is no evidence that the sick policyholder had failed to disclose a relevant preexisting condition. Congress heard, for instance, about a Texas nurse who lost coverage after a diagnosis for aggressive breast cancer. The reason? She had not disclosed a past visit to a dermatologist for acne.
A man with stage four non-Hodgkin type lymphoma lost his coverage as he was about to receive a stem-cell implant. The company pounced because a doctor had once noted in the patient’s file that a scan had shown a small aneurysm and some gallstones. The doctor had not informed the patient.
“Overall, what we have found is that the market for individual health insurance in the United States is fundamentally flawed,’’ said Representative Henry Waxman of California in a supreme understatement.
Despite these flaws, too many in Congress want to entrust the industry with coverage of the 47 million uninsured. Worse, they want to protect private insurers from competition from a Medicare-like public option for those who cannot get coverage through their employers. Presumably, a health reform law would include provisions banning the worst abuses, but as the three executives - from UnitedHealth’s Golden Rule Insurance Co., Assurant Health, and WellPoint Inc. - so baldly show, the yardstick of a public plan to measure the rest of the industry is a crucial protection.
Administrators of a public plan would hear from Congress in a heartbeat if they ever treated policyholders the way private insurers have. A Texas congressman did finally hear from the breast-cancer patient with acne who was denied coverage on a Friday last June for a mastectomy planned for that next Monday. By the time the congressman got the company to reinstate the policy it was October. The tumor had doubled in size and the surgeon had to remove all the lymph nodes in the woman’s arm.
If Congress can’t afford to provide uninsured Americans coverage as generous as its own, it should at least join President Obama and Senator Edward Kennedy and insist on a public-plan option.
---------
Health care reform - Examiner.com
Sandra Miller - Hampton Roads Women's Business Examiner - July 4, 2009
The average American spends more a year on health care than they do educating their children, building roads, and even feeding ourselves. It is estimated that we spent 2.6 trillion dollars in 2009, or $8,300.00 per person on health care. Forty five million Americans have no health insurance. Of course we all know that this is at the heart of the current debate on health care reform. There is a need to control costs while providing coverage for all.
John Lumpkin, MD, MPH, and director of the Health Care Group for the Robert Wood Johnson Foundation stated, "There is enough evidence that it is now time to do something and to do the right thing." There are many myths floating around regarding health care reform. There is a need to focus on the facts and to get rid of the myths. The myths are blocking our progress with regard to health care reform.
Here are a few of the myths:
Health care reform will not benefit me because I have insurance. Just because you have health insurance today, doesn't mean that you will have it tomorrow. According to the National Coalition on Health care, almost 266,000 companies dropped their employees' coverage from 2000 to 2005. "People with insurance have a stake because their insurance is at risk", says Judy Feder, a professor of public policy at Georgetown University. Judy is also a senior fellow at the Center for American Progress, a Washington, D. C. based think tank. In addition, in recent years the average employee health insurance premium rose nearly eight times faster than income. Stephanie Cathcart, spokesperson for the National Federation of Independent Business (NFIB), states "everyone is paying for health increases in some way, and it's unsustainable for everyone". "Reform will benefit everyone as long as it addresses costs."
Baby boomer's will bankrupt Medicare. This is another myth. If you want to blame the rise in health care costs on baby boomer's you need to look somewhere else. The growing ranks of the elderly only account for .4 percent of the future growth in health care costs, says Paul Ginsburn, president of the Center for Studying Health System Change. So why are costs in health care skyrocketing? Ginsburg and others point to all the fancy new technology. This is true. Someone has to pay for this new equipment that hospitals and doctors offices acquire. As with any business this cost is passed along to the consumer. We have MRI machines, CT scanning devices, new mammogram machines. As with any new technology when it first comes out it is expensive and then the cost goes down. Look at the computer. You can now purchase a brand new laptop for about $350.00. Years ago they ran about $2000.00. In addition, we have the fee for service payment system. This means that doctors are paid by the number of patients they see, and how many treatments they provide, rather than by the quality of care they provide. Some say this fee for service payment system encourages over treatment. This topic was discussed in the July-August 2008, edition of AARP the Magazine. You can view this article at aarpmagazine.org/health/health.care.costs.html.
Health care reform will cost us more. We have to think of health care reform as if it's an Energy Star appliance. It will cost more to replace your old energy guzzling refrigerator with a new one, but over time the savings will be substantial. The Commonwealth Fund, a New York City based foundation that supports research on health care practice and policy, estimates that health care reform will cost approximately 600 billion to implement, but by 2020 it could save us approximately 3 trillion.
My access to quality health care will decline. Just because you have access to lots of doctors that prescribe lots of treatments doesn't mean that you are getting quality care. Researchers at Dartmouth College found that patients who receive more care actually fare worse than those who receive less care. One example is heart attack patients. Heart attack patients in Los Angeles spent more days in the hospital and had more tests and procedures than heart attack patients in Salt Lake City, Utah. However, the patients in Los Angeles died at a higher rate than those in Salt Lake City. In addition, Medicare paid $30,000 for the Los Angeles patients, while they paid $23,000 for the Salt Lake City patients, who had better outcomes.
I won't be able to visit my favorite doctor. People worry that they will have fewer options when you start talking about health care reform. In our current system newer treatments are replacing older forms of treatment. It has been shown that the newer, more expensive treatments don't work any better than the older forms of treatment. One example of this is blood pressure medication. Doctors routinely prescribe new medications for treating blood pressure problems and the new medications are more expensive. Studies show that the older medications work just as well, if not better, and they are less expensive. New technology is a value, but in our current health care system there is no way to weigh whether these treatments work. There is currently comparative effectiveness research (CER) on which treatments work and which ones don't work. There are 18 organizations that support CER, including AARP, NFIB, Consumers Union, and Families USA. They believe that instead of limiting choices, health care reform will give doctors the information they need to practice better medicine. In our current system they are saying that expensive treatments replace less expensive ones for no reason.
The uninsured actually have access to good care in the emergency room. This is true. For five years while I was waiting to be approved by Social Security Disability, I had to use the emergency room and free clinics. You can get health care in this country if you are sick and in need of medical attention and you do not have to pay for it if you can not afford the bill. My quality of care was no less than it would have been if I had insurance, I always received excellent care. However, the emergency room alone does not help you get the right information to prevent a condition, or give you help in managing your condition, says Maria Ghazal, director of public policy for Business Roundtable, which is an association of Chief Executive Officers at major US companies. Forty one percent of the uninsured have no access to preventive care, so when they do go to the ER it is at a time when their illness has progressed and costs more to treat. According to Lumpkin Hospitals there is no way to recoup the costs of treating the uninsured, so they pass some of these costs on to the consumer that has insurance.
We can't afford to tackle this problem now. Although we are in the middle of a recession the most expensive thing we can do is nothing, according to Robert Zirkelbach, a spokesperson for America's Health Insurance Plans. If we do nothing the Congressional Budget Office projects that our annual health costs will rise to about $13,000 per person in 2017. In addition, the number of uninsured will rise to 54 million by 2019. More than half of Americans say they have cut back on health care in the past year due to cost concerns. Almost one in four of us have put off care that is needed, and one in five of us did not fill a prescription. The urgency for health care reform is greater now than it has ever been.
We will end up with socialized medicine. Some experts are in favor of a single payer system similar to Medicare or the health program offered to federal government employees. However, all of the proposals being offered now would build on our current system, which was an idea initiated by Hillary Clinton. Personally, I think this idea is the best and the most cost effective. Lumpkin Hospitals states, "there are many ways to solve our health care problem, but we will come up with a uniquely American solution, and that solution will be a mixed public and private solution."
---------
-

-
Karen Ignagni is CEO of America's Health Insurance Plans, the main health insurance lobby. She pushes for a bill that has no public option but that does require insurance for all. (Manuel Balce Ceneta/ Associated Press)
-
"Insurance figure at center of health debate: Lobby’s CEO adds a diplomatic voice"
By Lisa Wangsness, Boston Globe Staff, June 30, 2009
WASHINGTON - The face of the insurance industry in Washington is a slight, soft-spoken former AFL-CIO employee benefits director with a penchant for data-driven logic. She has the confidence and intellectual agility of a skilled debater, but prefers to dwell on areas of agreement. On healthcare, Karen Ignagni often sounds like the lifelong Democrat that she is.
“The president is right,’’ she said at a panel discussion recently, when asked about President Obama’s belief that insurers must stop refusing to cover people who are sick. “That needs to change.’’
It is no accident that Ignagni is the chief executive of America’s Health Insurance Plans, the main health insurance lobby, at a time when a popular new Democratic president is planning a sweeping healthcare overhaul. Insurance executives believe this may be a life-or-death moment: If Congress creates the strong government insurance option that liberals want, insurers say they would be unable to compete and would eventually go out of business.
On the other hand, if lawmakers pass a healthcare bill that has no public insurance alternative but that does require everyone to obtain insurance - and provides subsidies to help them afford it - the industry could pick up millions of new subscribers.
Standing at the precipice is Ignagni (pronounced ig-NAHN-ee), a 55-year-old native of Providence who has run AHIP for a half dozen years, earning her board’s loyalty by picking her battles wisely - and winning them. In the late 1990s, when she ran one of the group’s predecessor organizations, she helped defeat the Patient’s Bill of Rights by arguing that it would drive up premiums for workers; recently she helped insurers gain credibility with Democrats by supporting an expansion of public health insurance programs for children.
Andrew Stern, president of the Service Employees International Union, calls her “extremely effective’’ and says she is sometimes underestimated.
“She seems like a very nice, charming person; she rarely draws lines with people, and she always tries to engage people in what they’re thinking and explain herself very professionally,’’ he said. “But underneath that is a calculating, shrewd, capable person, in the best sense of the word, for her association.’’
Under Ignagni’s leadership, the industry has taken a strikingly different approach to reform than it did in 1993-94, when it sponsored the “Harry and Louise’’ ads that played a critical role in defeating the Clinton administration’s healthcare plan.
Times have changed since then: Medical costs have soared, doubling premiums in the last nine years and causing insurers to lose customers. The financial crisis and related scandals have provoked a backlash against the private sector. With a resurgent Democratic Party determined to win the elusive healthcare overhaul it has wanted for generations, Ignagni understands the threat to big insurance is grave indeed.
“The bar is high. American people want to hear solutions from private sector organizations and industries,’’ Ignagni said in an interview in her office, just down Pennsylvania Avenue from the White House.
Over the last three years, with the help of like-minded board members, Ignagni has helped convince her industry that merely standing in opposition would be a dangerous risk. She has also shown them, with financial analyses of the effect Massachusetts’ 2006 reforms have had on insurers, that the right changes could help the industry not just survive but prosper.
“She has, by her intellect and by force of personality, led these pretty powerful executives to understanding both that they can participate in what is going on and that they should, because their companies will survive if the Congress and the White House understand what’s necessary to give people private insurance choices,’’ said James Roosevelt, CEO of Tufts Health Plan and a member of the AHIP board.
A month before Obama’s inauguration, AHIP declared its support for major market reforms, agreeing to stop refusing to cover sick people as long as Congress requires all Americans to obtain insurance. It backed up this position with a surprisingly detailed healthcare plan showing how these market reforms could help deliver universal coverage. It was a radical move within the industry, which has long maintained its profit margins by seeking out healthy customers and avoiding people with preexisting conditions. AHIP upped its ante this spring, promising to stop pricing premiums according to health status, a practice known as medical underwriting, as long as everyone has to buy insurance.
For more than a year, Ignagni has also met with other healthcare industries and consumer groups in a search for common ground, hoping to stave off a more fundamental restructuring of the health system.
“They can’t afford to see the movement for single payer grow,’’ said John Rother, legislative and policy director for AARP. “I think Karen is smart to be repositioning the industry on the side of reform.’’
But as the healthcare debate intensifies, Ignagni is walking a fine line between emphasizing the industry’s support for universal coverage and issuing dire warnings against the “unintended consequences’’ of a public health insurance plan. A strong national public insurance option would underpay doctors and hospitals, leaving them to shift more costs onto private payers, she says. Then, the insurance industry would collapse, flooding the government with billions of dollars in new obligations.
“A government-run plan - no matter how it is initially structured - would dismantle employer-based coverage, significantly increasing costs for those who remain in private coverage, and add additional liabilities to the federal deficit,’’ she wrote last week to the leaders of the Senate health committee.
Critics on the left, including the president himself, disagree. “If private insurers say that the marketplace provides the best quality healthcare . . . then why is it that the government - which they say can’t run anything - suddenly is going to drive them out of business?’’ Obama said at his news conference last week. “That’s not logical.’’
Though she is the voice of a wealthy industry, Ignagni comes from a family of union municipal workers. Her father was a firefighter and her mother administered grants at Providence City Hall. She can remember rolling down the steep Rhode Island State House lawn as a child, when her grandmother, a maintenance worker, lived across the street.
Not long after graduating from Providence College, Ignagni worked for a liberal healthcare advocacy group in Washington and later for the AFL-CIO, where she spent 11 years helping unions preserve their health benefits in the face of rapidly rising costs. From there she joined an association of HMOs, and when that group merged with a for-profit insurers’ lobby in the mid-1990s, the new board chose her as its leader.
Ignagni says she sees no ideological dissonance between her past and present views of the insurance industry. She says she has always believed that efficient, appropriate care is the best way to keep costs down and to ensure universal access. That is precisely the value she says the insurance industry has shown it can add through innovative programs like paying doctors for higher quality and helping people control their chronic diseases. The government, she argues, has failed to do the same in Medicare.
She acknowledges that the industry has made mistakes. A few days after Obama retold the story of how his dying mother spent her final days fighting with her insurance company, which insisted her ovarian cancer was a preexisting condition, Ignagni told a healthcare breakfast on Capitol Hill: “The president and his mother lived through something that we have worked so hard to prevent . . . we can get legislation to make sure that never happens to a family in this country again.’’
It remains unclear whether the insurance industry has delayed making such acknowledgments for too long. Ignagni says she is reading “Fiasco,’’ Thomas Ricks’s account of the mistakes the US military made in Iraq.
“I think that every CEO ought to read books like that,’’ she said, “because it’s a story about missed opportunities and wrong decisions.’’
-
Lisa Wangsness can be reached at lwangsness@globe.com.
-
---------
-

-
The emergency room waiting area at Coney Island Hospital in Brooklyn. The hospital's emergency room receives about 60,000 patients a year. (Getty Images / Mario Tama)
-
"Healthy examples: Plenty of countries get healthcare right."
By Jonathan Cohn, The Boston Globe, IDEAS, July 5, 2009
“I DON’T WANT America to begin rationing care to their citizens in the way these other countries do.”
That was Arizona Senator Jon Kyl, speaking last month about healthcare reform. But it could have been virtually any other Republican, not to mention any number of sympathetic interest groups, because that’s the party line for many who oppose healthcare reform. If President Obama and his supporters get their way, this argument goes, healthcare in America will start to look like healthcare overseas. Yes, maybe everybody will have insurance. But people will have to wait in long lines. And when they are done waiting in line, the care won’t be very good.
Typically the people making these arguments are basing their analysis on one of two countries, Canada and England, where such descriptions hold at least some truth. Although the people in both countries receive pretty good healthcare - their citizens do better than Americans in many important respects - they are also subjected to longer waits for specialty care and tighter limits on some advanced treatments.
But no serious politician is talking about recreating either the British or the Canadian system here. The British have truly “socialized medicine,” in which the government directly employs most doctors. The Canadians have one of the world’s most centralized “single-payer” systems, in which the government insures everybody directly and private insurance has virtually no role. A better understanding for how universal healthcare might work in America would come from other countries - countries whose insurance architecture and medical cultures more closely resemble the framework we’d likely create here.
Last year, I had the opportunity to spend time researching two of these countries: France and the Netherlands. Neither country gets the attention that Canada and England do. That might be because English isn’t their language. Or it might be because they don’t fit the negative stereotypes of life in countries where government is more directly involved in medical care.
Over the course of a month, I spoke to just about everybody I could find who might know something about these healthcare systems: Elected officials, industry leaders, scholars - plus, of course, doctors and patients. And sure enough, I heard some complaints. Dutch doctors, for example, thought they had too much paperwork. French public health experts thought patients with chronic disease weren’t getting the kind of sustained, coordinated medical care that they needed.
But in the course of a few dozen lengthy interviews, not once did I encounter an interview subject who wanted to trade places with an American. And it was easy enough to see why. People in these countries were getting precisely what most Americans say they want: Timely, quality care. Physicians felt free to practice medicine the way they wanted; companies got to concentrate on their lines of business, rather than develop expertise in managing health benefits. But, in contrast with the US, everybody had insurance. The papers weren’t filled with stories of people going bankrupt or skipping medical care because they couldn’t afford to pay their bills. And they did all this while paying substantially less, overall, than we do.
The Dutch and the French organize their healthcare differently. In the Netherlands, people buy health insurance from competing private carriers; in France, people get basic insurance from nonprofit sickness funds that effectively operate as extensions of the state, then have the option to purchase supplemental insurance on their own. (It’s as if everybody is enrolled in Medicare.) But in both countries virtually all people have insurance that covers virtually all legitimate medical services. In both countries, the government is heavily involved in regulating prices and setting national budgets. And, in both countries, people pay for health insurance through a combination of private payments and what are, by American standards, substantial taxes.
You could be forgiven for assuming, as Kyl and his allies suggest, that so much government control leads to Soviet-style rationing, with people waiting in long lines and clawing their way through mind-numbing bureaucracies every time they have a sore throat. But, in general, both the Dutch and French appear to have easy access to basic medical care - easier access, in fact, than is the American norm.
In both the Netherlands and France, most people have long-standing relationships with their primary care doctors. And when they need to see these doctors, they do so without delay or hassle. In a 2008 survey of adults with chronic disease conducted by the Commonwealth Fund - a foundation which financed my own research abroad - 60 percent of Dutch patients and 42 percent of French patients could get same-day appointments. The figure in the US was just 26 percent.
The contrast with after-hours care is even more striking. If you live in either Amsterdam or Paris, and get sick after your family physician has gone home, a phone call will typically get you an immediate medical consultation - or even, if necessary, a house call. And if you need the sort of attention available only at a formal medical facility, you can get that, too - without the long waits typical in US emergency rooms.
This is particularly true in the Netherlands, thanks to a nationwide network of urgent care centers the government and medical societies have put in place. Not only do these centers provide easily accessible care for people who use them; they leave hospital emergency rooms free to concentrate on the truly serious cases. Tellingly, a Dutch physician I met complained to me that waiting times in her emergency room had been getting “too long” lately. “Too long,” she went on to tell me, meant two or three hours. When I told her about documented cases of people waiting a day, or even days, for treatment in some American emergency rooms, she thought I was joking. (In a 2007 Commonwealth Fund survey, just 9 percent of Dutch patients reported waiting more than two hours for care in an ER, compared to 31 percent of Americans.)
Dutch and French patients do wait longer than Americans for specialty care; around a quarter of respondents to the Commonwealth Fund survey reported waiting more than two months to see a specialist, compared to virtually no Americans. But Dutch and French patients were far less likely to avoid seeing a specialist altogether - or forgoing other sorts of medical care - because they couldn’t afford it. And there’s precious little evidence that the waits for specialty care led to less effective care.
On the contrary, the data suggests that while American healthcare is particularly good at treating some diseases, it’s not as good at treating others. (In some studies, the US did pretty well on cardiovascular care, not so well on diabetes, for example.) Overall, the US actually fares poorly on measures like “potential years of lives lost” - statistics compiled by specialists in an effort to measure how well healthcare systems perform. In a 2003 ranking of 20 advanced countries, the US finished 16th when it came to “mortality amenable to healthcare,” another statistic that strives to capture the impact of a health system. The Dutch were 11th and the French were fifth. These statistics are necessarily crude; diet, culture, and many other factors inevitably affect the results. But, taken together, they make it awfully hard to argue that care in these countries is somehow inferior. If anything, the opposite would seem to be true.
Critics of health reform frequently point to cancer as proof that American healthcare really is superior. And, it’s true, the US has, overall, the world’s highest five-year survival rate for cancer. But that’s partly a product of the unparalleled amount of government-funded research in the US - something healthcare reform would not diminish. Besides, it’s not as if the gap is as large or meaningful as reform critics frequently suggest. France (like a few other European countries) has survival rates that are generally close and, for some cancers, higher. Much of the remaining difference reflects differences in treatment patterns that have nothing to do with insurance arrangements and everything to do with idiosyncratic medical cultures. This is particularly true of prostate cancer, where a staggeringly high survival rate in the US seems to be largely a product of aggressive US treatment - treatment that physicians in other countries, and increasingly many specialists here, consider unnecessary and sometimes harmful.
None of this is to say that either the Dutch or French systems are perfect. Far from it. In both countries, healthcare costs are rising faster than either the public - or the country’s business interests - would like. And each country has undertaken reforms in an effort to address these problems. The French have started to introduce some of the managed care techniques familiar to Americans, like charging patients extra if they see specialists without a referral, while developing more evidence-based treatment guidelines in the hope that it will reduce the use of unnecessary but expensive treatments. The Dutch overhauled their insurance arrangements a few years ago, to introduce more market competition and reward healthcare providers - that is, doctors and hospitals - who get good results.
But cost is the one area in which France and the Netherlands are a lot like Canada and England: They all devote significantly less of their economy to healthcare than we do. The French spend around 11 percent of their gross domestic product on healthcare, the Dutch around 10. In the US, we spend around 16 percent. And, unlike in the US, the burden for paying this is distributed across society - to both individuals and businesses - in an even, predictable way.
Of course, reforming health insurance in the US isn’t going to turn this country into France or the Netherlands overnight, any more than it would turn the US into Britain and Canada. The truth is that the changes now under consideration in Washington are relatively modest, by international standards. But insofar as countries abroad give us an idea of what could happen, eventually, if we change our health insurance arrangements, the experience of people in Amsterdam and Paris surely matters as much as - if not more than - those in Montreal and London. In those countries, government intervention has created a health system in which people seem to have the best of all worlds: convenience, quality, and affordability. There’s no reason to think the same thing couldn’t happen here.
-
Jonathan Cohn is a senior editor of The New Republic, where he writes a blog called “The Treatment.” He is also the author of “Sick: The Untold Story of America’s Health Care Crisis - and the People Who Pay the Price (HarperCollins, 2007).
-
---------
"POLITICAL NOTEBOOK: Healthcare firms load up on lobbyists"
Boston.com - By Associated Press, July 7, 2009
WASHINGTON - The nation’s largest insurers, hospitals, and medical groups have hired more than 350 former government staff members and retired members of Congress in hopes of influencing their old bosses and colleagues, according to an analysis of lobbying disclosures and other records.
The tactic is so widespread that three of every four major healthcare firms have at least one former insider on their lobbying payrolls, according to The Washington Post’s analysis.
Nearly half of the insiders previously worked for the key committees and lawmakers, including Senators Max Baucus, a Montana Democrat, and Charles Grassley, an Iowa Republican, that are debating whether to adopt a public insurance option opposed by major industry groups. At least 10 others have been members of Congress, such as former House majority leaders Richard Armey, a Texas Republican, and Richard Gephardt, a Missouri Democrat, both of whom represent a New Jersey pharmaceutical firm.
The hirings are part of a record-breaking influence campaign by the healthcare industry, which is spending more than $1.4 million a day on lobbying in the current fight, according to disclosure records. Overall, healthcare companies and their representatives spent more than $126 million on lobbying in the first quarter, leading all other industries, according to Senate data and the Center for Responsive Politics.
The television ad wars are also beginning and expected to grow this summer.
Through June 27, $31 million was spent for roughly 47,000 TV ads on healthcare this year, said Evan Tracey, president of the Campaign Media Analysis Group, a firm that tracks issue advertising. That’s double the roughly $14 million the insurance industry spent in 1993 and 1994 for the famous “Harry and Louise’’ ads credited with helping kill President Clinton’s healthcare drive, but a fraction of the $250 million Tracey guesses will ultimately be spent this year.
So far about $15 million has been spent on ads favoring the Democrats’ push to revamp healthcare, and $4 million to oppose it. Another $12 million has gone to ads generally favoring better healthcare - nearly all of that was spent by the Pharmaceutical Research and Manufacturers of America, representing drug makers, which hopes its market will expand.
---------
"Comparing the bills"
Boston.com - July 17, 2009
Summaries of the healthcare overhaul measure three House committees worked on yesterday and the bill passed Wednesday by the Senate health committee:
Who’s covered
House: About 94 percent of non-elderly residents (those not covered by Medicare, which takes effect kicks in at age 65), compared with 81 percent today.
Senate: Aims to cover 97 percent of Americans.
Cost
House: About $1.5 trillion over 10 years.
Senate: About $615 billion over 10 years, but is only one piece of a larger Senate bill.
Financing
House: $544 billion from a new income tax surcharge on single people making $280,000 or more a year and on couples making $350,000 and above; about $500 billion in cuts to Medicare and Medicaid; about $200 billion from penalties paid by individuals and employers who don’t obtain coverage.
Senate: Undetermined; Senate Finance Committee is responsible for financing.
Requirements for individuals
House: Must have insurance, enforced through tax penalty of 2.5 percent of income. Some hardship waivers available.
Senate: Similar provisions.
Requirements for employers
House: Must provide insurance to their employees or pay a penalty of 8 percent of payroll. Companies with payroll under $250,000 annually are exempt.
Senate: Employers who don’t offer coverage pay a penalty of $750 a year for each full-time worker. Businesses with 25 or fewer workers are exempted.
Subsidies
House: Individuals and families with annual income up to 400 percent of poverty level ($88,000 for a family of four) would get help buying coverage.
Senate: Similar provisions.
Choosing insurance
House: Through a new Health Insurance Exchange open to individuals and, initially, small employers. States could operate exchanges if they follow federal rules.
Senate: Individuals and small businesses could buy insurance through state-based purchasing pools.
Public insurance plan
House: New Public plan available through the insurance exchanges would be set up and run by the secretary of health and human services. On average, it would pay Medicare rates plus 5 percent to doctors.
Senate: New public plan to compete with private insurers that would be run by the government, but would pay doctors and hospitals based on what private insurers now pay.
Benefits
House: Preventive services, mental health services, oral heath, and vision for children. Out-of pocket costs would be capped, and insurers would be barred from denying coverage based on pre-existing conditions.
Senate: Similar provisions.
Associated Press
---------
mid-July of 2009
-

-
---------
"Industry Cash Flowed To Drafters of Reform: Key Senator Baucus Is a Leading Recipient"
By Dan Eggen, Washington Post Staff Writer, Tuesday, July 21, 2009
As liberal protesters marched outside, Sen. Max Baucus sat down inside a San Francisco mansion for a dinner of chicken cordon bleu and a discussion of landmark health-care legislation under consideration by his Senate Finance Committee.
At the table on May 26 were about 20 donors willing to fork over $10,000 or more to the Democratic Senatorial Campaign Committee, including executives of major insurance companies, hospitals and other health-care firms.
"Most people there had an agenda; they wanted the ear of a senator, and they got it," said Aaron Roland, a San Francisco health-care activist who paid half price to attend the gathering. "Money gets you in the door. The only thing the other side can do is march around and protest outside."
As his committee has taken center stage in the battle over health-care reform, Chairman Baucus (D-Mont.) has emerged as a leading recipient of Senate campaign contributions from the hospitals, insurers and other medical interest groups hoping to shape the legislation to their advantage. Health-related companies and their employees gave Baucus's political committees nearly $1.5 million in 2007 and 2008, when he began holding hearings and making preparations for this year's reform debate.
Top health executives and lobbyists have continued to flock to the senator's often extravagant fundraising events in recent months. During a Senate break in late June, for example, Baucus held his 10th annual fly-fishing and golfing weekend in Big Sky, Mont., for a minimum donation of $2,500. Later this month comes "Camp Baucus," a "trip for the whole family" that adds horseback riding and hiking to the list of activities.
To avoid any appearance of favoritism, his aides say, Baucus quietly began refusing contributions from health-care political action committees after June 1. But the policy does not apply to lobbyists or corporate executives, who continued to make donations, disclosure records show.
Baucus declined requests to comment for this article. Spokesman Tyler Matsdorf said the senator "is only driven by one thing: what is right for Montana and the country. And he will continue his open process of working together with the president, his colleagues in Congress, and groups and individuals from across the nation to get this legislation passed."
Baucus's fundraising prowess underscores the enduring political strength of the health-care lobby, which led all other sectors in donations to federal candidates during the last election cycle and has shifted its giving to Democrats as the party has tightened its control of Congress.
The sector gave nearly $170 million to federal lawmakers in 2007 and 2008, with 54 percent going to Democrats, according to data compiled by the Center for Responsive Politics, which tracks money in politics. The shift in parties was even more pronounced during the first three months of this year, when Democrats collected 60 percent of the $5.4 million donated by health-care companies and their employees, the data show.
Many of these contributions have been focused on Baucus, Charles E. Grassley (R-Iowa) and other senators in the moderate camps of their respective parties, whose votes could prove crucial in a final health-care reform deal, as well as the leaders of five key committees leading the debate. Grassley, the Finance Committee's ranking Republican, received more than $2 million from the health and insurance sectors since 2003. House Ways and Means Chairman Charles B. Rangel (D-N.Y.) took in $1.6 million from the health sector and its employees over the past two years; ranking Republican Dave Camp (Mich.) received nearly $1 million.
But Baucus, a senator from a sparsely populated and conservative Western state who is serving his sixth term, stands out for the rising tide of health-care contributions to his campaign committee, Friends of Max Baucus, and his political-action committee, Glacier PAC. Baucus collected $3 million from the health and insurance sectors from 2003 to 2008, about 20 percent of the total, data show. Less than 10 percent of the money came from Montana.
Top out-of-state corporate contributors included Schering-Plough, New York Life Insurance, Amgen, and Blue Cross and Blue Shield; individual executives such as Richard T. Clark, chief executive and president of drugmaker Merck, have also made regular donations. Most of these companies, particularly major insurers, strongly oppose a public insurance option, which is favored by President Obama and top House Democrats but has not received support from Baucus's committee.
Baucus is a longtime centrist in the Democratic caucus, and his committee chairmanship has made him a key broker in the health-reform debate. Many former Baucus staff members, including two chiefs of staff, lobby on behalf of the pharmaceutical industry and other health-care players and have been closely involved in negotiations on the legislation.
John Jonas, a Patton Boggs health-care lobbyist who has attended a Baucus fly-fishing event and other fundraisers, said the Montana senator is "key to getting anything done" when it comes to health-care legislation.
"This is not an overwhelmingly liberal Congress, and it's certainly not a liberal Senate," said Jonas, whose clients include Bristol-Myers Squibb, Pfizer and Northwestern Mutual. "I think Max is uniquely situated to try to accomplish that, because he's more of a centrist and moderate Democrat than others are."
But Jerry Flanagan, a health-care analyst with Consumer Watchdog, a California-based advocacy group, said the tide of campaign contributions amounts to "a huge down payment" by companies that expect favorable policies in return. "That is the cold reality of big-money politics," he said.
Baucus won easy reelection in the fall, but he has continued to hold fundraisers since then. In addition to the fly-fishing event, he held his "Eighth Annual Ski and Snowmobile Weekend" in Big Sky in February and celebrated the start of his sixth term with a $10,000-a-table dinner at the Washington Court Hotel later that month. Aides say another fundraiser scheduled for July 7 at Bistro Bis in Capitol Hill was scrapped.
Baucus's office declined to provide attendance and donation details about his fundraising events, and federal records laws do not require such disclosures. Starting in June, aides say, Baucus adopted an internal office policy to refuse contributions from health-care PACs and to continue doing so until after Congress passes reform legislation.
But new Federal Election Commission documents filed last week show that individual lobbyists and others with health-care connections continued to make contributions to Baucus committees throughout June. Examples from Baucus's Glacier PAC include $5,000 from the Independent Insurance Agents and Brokers of America and $2,500 from lobbyists with U.S. Strategies, which represents numerous health-care firms. Overall, half of the $110,000 in donations to the PAC from April to June came from health-care firms and lobbyists, including Schering-Plough, Medtronic and New York Life.
Craig Holman, government affairs lobbyist for the Public Citizen advocacy group, said the continued fundraising by Baucus during the health-care debate is "very troubling."
"He's doing all this fundraising right in the middle of this effort to mark up a bill," Holman said. "When you put these events close to matters concerning these lobbyists, clearly it's a signal. You are expected to show up with a check."
Baucus and his aides strongly dispute any assertion that campaign contributions have an impact on the senator's policy views and proposals. Aides say he has frequently backed policies opposed by health-care companies, including support for greater availability of generic drugs, allowing drug imports from Canada and cutting payments to the Medicare Advantage plan.
During an interview earlier this year with the Missoulian newspaper, Baucus said that "no one gets special treatment." He added: "Your word is your bond back there."
-
Research editor Alice Crites contributed to this report.
-
---------
The Boston Globe, Op-Ed
DAVID OSBORNE
"Healthcare blinders"
By David Osborne, July 24, 2009
FOR DECADES, outdated ideologies have hamstrung national politics. Now it’s happening again: Healthcare reform threatens to derail over the burning question of whether we need another public program. This is a massive diversion.
If structured correctly, a new public program could help transform the healthcare marketplace. But if it’s Medicare-for-all, with fee-for-service reimbursement, it could intensify the rate of healthcare inflation and make universal coverage unsustainable. The crucial issue is not public or private. It is the incentives and performance standards built into the system. If we don’t change those, we’re sunk.
Put simply, we must change the way we pay for care. The financial incentives in our system are backwards. Under fee-for-service payment, providers make more money by performing more services. If a hospital makes a mistake and the patient has to be treated again, the hospital makes more money. If a provider group figures out economical ways to keep patients healthy, it starves.
When the incomes of doctors and hospitals are squeezed, they do more procedures. Research by John Wennberg and Elliott Fisher at Dartmouth University shows that regions with more doctors per capita have higher rates of hospitalization and procedures - often twice the level of regions with fewer doctors. Yet this higher spending yields worse outcomes!
Wennberg says that up to a third of the $2.4 trillion spent on healthcare each year is wasted on unnecessary treatments, overpriced drugs, and end-of-life care.
Wennberg’s research also shows that integrated, managed healthcare providers are more efficient. Regions dominated by such providers have costs that are up to one-third lower than in other areas, because those providers use “evidence-based standards of care,’’ electronic records, and other methods to keep costs down and quality up.
We need to replace fee-for-service reimbursement with price competition between integrated providers that are paid by the year, not the procedure. They, in turn, should pay their doctors and hospitals lump sums for cycles of treatment for medical conditions - such as a knee replacement or a year’s treatment of diabetes. In Massachusetts, a commission created by the Legislature recommended a shift to such “global payments.’’
The outcomes of that care should be measured and reported to buyers (including health plans, consumers, employers, and public programs like Medicare and Medicaid), so they can make choices based on both price and quality.
How do we get there? First, Medicare should shift to this kind of “global payment’’ system.
Second, federal reform should empower states (and multi-state regions) to create purchasing exchanges involving all their public programs - Medicaid, the State Children’s Health Insurance Program, government employees’ and retirees’ plans, and subsidized insurance - plus private employers willing to join the pool. States would then invite health plans to compete for this market.
Wisconsin’s insurance program for state employees shows how this could work. The program defines a basic benefit package, asks health plans to submit bids specifying the annual dollar amount they would charge for this package, then ranks the bids into three tiers.
Low-price, high-quality plans, ranked in tier one, cost the least for state employees. If employees prefer a tier-two or -three plan - because their physician is not part of a tier-one plan, for instance - they are free to choose it and pay part of the difference. But the majority of members choose tier-one plans, and this helps keep prices down.
Wisconsin put this approach into effect in 2003. In Dane County, which includes the state capitol, the employee plan covers 25 percent of the private market. By 2006, state employee costs for individual and family plans in Dane County had fallen 14 percent below the statewide average and 30 percent below the most expensive regions. This has in turn slowed rising costs among private market providers in the county, compared with the rest of the state.
Let’s drop our ideological blinders and admit that adding one more public program will not solve all our problems (nor destroy the system). To get quality care for all at a price we can afford, we have to change the incentives and standards operating within medicine.
-
David Osborne is co-author of “Reinventing Government,’’ “The Price of Government,’’ and a chapter on reinventing healthcare in “Memos to the New President.’’
-
---------
Op-Ed: "Health care status quo would be disaster for middle class"
By House Majority Leader Steny Hoyer (D-MD), Monday, July 27, 2009
Washington, DC — How’s this for a health care plan? It will make your premiums go up—in fact, it will double health costs over the next ten years. It will strip millions of Americans of their coverage. It will send our deficit through the roof.
That, as President Obama recently pointed out, is the health care plan we choose by doing nothing. That is the status quo, and it will be the health care plan we end up with if health insurance reform fails.
And although no one will come out and argue for a plan that doubles costs and cuts coverage, we are being pushed in just that direction by transparent attempts to kill reform for partisan gain. As one Republican Senator put it, “If we’re able to stop Obama on this, it will be his Waterloo. It will break him.” Another said this about efforts to cover millions more Americans: “We can stall it. And that’s going to be a huge gain for those of us who want to turn this thing over in the 2010 election.”
Failure to reform health care might be a boon for some members of Congress, but it would be a disaster for middle-class families, for the 47 million uninsured Americans, and for small businesses across America.
That’s why Democrats are working hard to get a health care bill to President Obama’s desk this fall. The details of that bill are still under strong debate—which is healthy considering the historic challenge we face. But Democrats are unshakably committed to four driving principles: health insurance stability, affordability, quality, and patient choice.
First, we are working to bring stable coverage and peace of mind to every American. No longer will insurance companies be allowed to deny you coverage because they consider you to have a pre-existing condition like pregnancy, heart disease, cancer, or diabetes. No longer will medical bills be a source of personal bankruptcy. No longer will you be forced to make job and life choices based on fear of losing health coverage. And no longer will tens of millions without insurance be forced to put off the preventive care they need, while the rest of us pay to subsidize their care—at about $1,100 per average family premium, each year.
Second, the Democratic plan has the power to reverse the cost inflation that has more than doubled premiums since 2000, while wages have stood still. Cost-saving measures will include the bargaining power of a public insurance option, an end to Medicare co-pays or deductibles for preventive care that keeps patients healthier for the long-term, research to help doctors and patients make informed choices, and electronic medical records that will make it easier for doctors to collaborate. Seniors will see an end to the notorious Medicare Part D “donut hole,” which leaves those with between $2,700 and $6,100 per year in prescription drug expenses without Medicare support. And small businesses will find it easier to afford coverage for their employees, putting them on fairer footing against competitors overseas.
Third, the Democratic plan will mean higher-quality health care. Right now, America pays nearly twice as much for health care per capita as any other industrialized country, without getting better health outcomes in return. In other words, higher quality health care isn’t a matter of spending more money—it’s a matter of spending smarter. That’s why many of the same measures that will bring down costs can also mean better health care for all of us. For instance, electronic records will mean fewer deadly errors, and research on health outcomes will help patients and doctors decide on the most effective courses of treatment.
Fourth and finally, Democrats want to preserve and strengthen patients’ choice of plans and doctors. An option to enroll in a public insurance plan won’t simply give Americans another choice of coverage—its competition will push private insurers toward lower costs and higher quality. And contrary to Republican claims, the Democratic plan won’t force employers to drop millions of employers from coverage; the Congressional Budget Office actually found that employer-provided coverage will increase. As a result, Americans who like the coverage they have will be able to keep it.
Even as you’re reading this, we’re working with President Obama to finish a bill that will hold to the principles of stability, affordability, quality, and patient choice, without raising the deficit. The status quo is getting costlier every day, and that makes our work more urgent.
But anyone who seriously claims that we are rushing through reform needs a reality check. The House held 79 health care hearings in the last two years; just this year, members of Congress have heard from their constituents at more than 550 health care town halls and public events.
And not just that—for decades, health reform has been one of the most-discussed domestic issues in America. In the 2008 election, repairing the economy and expanding access to health care were central issues for all candidates, in both parties. In fact, we, as a nation, have been debating about how to bring affordable health care to every American for most of the 20th century, and into the 21st. This, at last, is our moment. We must not miss it.
-
Rep. Steny Hoyer (D-MD) is the House Majority Leader and a leading voice in the Democratic party. He is currently serving his 15th term representing the 5th Congressional District of Maryland.
-
---------
"Government plan can coexist with private insurance"
By Ricardo Alonso-zaldivar, Associated Press Writer, July 27, 2009
WASHINGTON – A new government health insurance plan sought by President Barack Obama and congressional Democrats could coexist with private insurers without driving them out of business, an analysis by nonpartisan budget experts suggests.
The estimate by the nonpartisan Congressional Budget Office — seen as good news by Democrats — comes as leaders pushed Monday to make progress on health care overhaul before lawmakers go home for their August recess.
House Speaker Nancy Pelosi, D-Calif., says a floor vote is still possible in the next few days, and Democrats called a meeting of all their House members late Monday afternoon. In the Senate, a small group of lawmakers from both parties were resuming negotiations in search of an elusive compromise.
Obama's ambitious timetable for his top domestic priority has slipped as Democratic dissension has slowed the legislative work.
The White House and congressional Democrats were angered two weeks ago when the budget office director, Douglas Elmendorf, told Congress that the House bill lacked mechanisms to bring health care costs under control.
Now, Democrats are using the budget office's suggestion that a government-run insurance plan would not destroy private insurers to rebut one of the main charges against their proposal — that it would lead to a federal takeover of the private health insurance marketplace.
The controversy seems far from settled, given uncertainty over projections of how a revamped health care system would work.
Polls have shown that Americans support the idea of a public coverage option as part of health care overhaul. The insurance industry and employer groups say it could drive private insurers out of business, particularly if the government plan had the power to pay medical providers below-market rates.
More than 160 million workers and family members now get health insurance through an employer. A widely cited study by the Lewin Group, a private health research firm, estimated that more than 100 million people would sign up for the public plan proposed by House Democrats, making it the dominant insurer in the land.
But the budget office, in a letter Sunday to a senior Republican lawmaker, said its own estimate for the same legislation is "substantially smaller."
CBO estimates that only 11 million to 12 million people would sign up for the public plan — making it a much smaller player in the market. The government coverage would be available alongside private plans through a new kind of insurance purchasing pool called an exchange. CBO estimated about 6 million of those enrolled in the public plan would be workers and family members of employers that joined the exchange.
The reasons the estimates are so far apart have to do with different underlying assumptions.
The CBO estimated that the public plan would offer premiums about 10 percent lower than private plans; the Lewin analysis estimates the premiums would be at least 20 percent lower. The CBO estimates that only individuals and workers in companies with fewer than 50 employees would join the exchange, while Lewin estimated the exchange would eventually be open to all workers.
As if to underscore how such estimates can vary, the Urban Institute public policy center also ran calculations — and came up with different numbers. The Urban Institute estimated that about 47 million people would sign up for the public plan, if companies with fewer than 50 workers were allowed to join.
---------
"Are big insurance discounts for healthy behavior unfair?"
By Mary Agnes Carey, Kaiser Health News, Monday, July 27, 2009
WASHINGTON — Employers and health insurers could give larger discounts to employees who lose weight or lower their cholesterol under one health care overhaul proposal that's moving through Congress .
However, the AARP , the American Heart Association and other groups think it's unfair and fear it could result in higher premiums for people who don't achieve those fitness goals.
The discounts are being pushed by Safeway chief executive Steve Burd , who said that rewarding healthy behavior has helped keep the Pleasanton, Calif. , supermarket chain's health care costs flat while other companies' have skyrocketed. He's met with several lawmakers on Capitol Hill .
The proposal, which involves the sensitive issue of how aggressive employers can be in trying to induce workers to change their behavior to reduce their risks of disease, draws skepticism from many patient advocates.
"If you give one person a discount, someone else is going to end up paying more," said Paul Cotton of AARP , one of more than 60 groups that's fighting the provision. "So the people who aren't able to change their behavior or participate in the program will end up paying more. Our fear is that premiums will become unaffordable for people who can't change their behavior."
Under current law, employers and insurers are permitted to give discounts of up to 20 percent on premiums, co-payments or deductibles to workers who take part in wellness programs, which include anti-smoking and weight-loss programs. Some wellness programs simply require participation in order to get the discount, but others require employees to reduce their weight, blood pressure or cholesterol by specific levels.
Health care overhaul legislation passed by the Senate Health, Education, Labor and Pensions Committee would allow employers to increase those discounts to 30 percent, and up to 50 percent if the secretaries of Labor, Health and Human Services and Treasury agree. A proposal in the House of Representatives would allow employers to charge workers who participate in wellness programs 50 percent less than workers who don't.
Proponents say that the measure would improve health and lower costs, and that workers who can't hit specific targets could seek a medical exemption.
"There is significant savings and significant positives to encouraging people to live healthy lifestyles and reward people monetarily for doing it," said Sen. Judd Gregg , R- N.H. , a co-sponsor of the amendment to the health committee bill. "That's just common sense and we should do it. If you create a healthier work force by incentivizing healthy lifestyles you reduce the overall cost of health care for everyone."
The groups fighting the provision say that while many employees might want to exercise and eat right, some might find that work schedules and family commitments prevent them from making the lifestyle changes needed to improve their health. Lower-income workers, in particular, might not be able to afford gym memberships, even with employers' subsidies.
"We are very concerned that individuals not be penalized — either financially or by exclusion from coverage or services — if they are sick or if they presently engage in specific behaviors or have certain health conditions, such as smoking or obesity," the groups wrote to Congress . The groups signing the letter include the American Diabetes Association , the American Lung Association , the American Federation of State, County and Municipal Employees and the American Cancer Society Cancer Action Network.
Some health advocates are more comfortable with linking financial incentives to other factors, such as refilling prescriptions or monitoring blood sugar on a regular basis, as opposed to meeting a specific fitness target.
"Once you get into paying more for specific outcomes, for many people that does cross over the line," said Ken Thorpe , executive director of the Partnership to Fight Chronic Disease, a coalition whose members include groups representing patients, health care providers and business and labor.
Employer groups are urging lawmakers to increase the discounts in premiums, co-pays and deductibles they can give to workers who participate in wellness programs.
"The value of health insurance premium discounts or rebates to promote employee participation in wellness programs has had and will continue to have a cost savings effect on multiple levels for our health care system," the groups, which include the Business Roundtable and the U.S. Chamber of Commerce , wrote to members of the House Energy and Commerce Committee . "They clearly motivate healthy behaviors as well as reduce health care costs."
A Senate GOP aide said the amendment includes language to prohibit any discrimination against individuals who can't attain specific fitness goals because of medical reasons or other factors. People who feel they can't meet the standards can request waivers or alternative standards from their employers. Employers can also ask for physician to certify that employees have existing medical conditions that would prevent them from meeting specific health goals. The programs must be "reasonable" and not "overly burdensome," open to all employees, and participation must be voluntary.
Safeway's Burd, whose company has given financial incentives to non-union employees to lose weight, cut tobacco use and reduce blood pressure and cholesterol levels, has said that obesity and smoking rates among employees in the voluntary program are roughly 70 percent of the national average. In the past four years, Burd has said, his company's health care costs have been flat "while most American companies' costs have increased 38 percent over the same four years."
By Safeway's calculations, "if the nation had adopted our approach in 2005, the nation's direct health-care bill would be $550 billion less than it is today," Burd wrote in a June 12 op-ed in The Wall Street Journal .
Critics say Burd's data haven't been independently verified. A Safeway spokeswoman acknowledged that there hasn't been an independent analysis, but "we were able to see savings clearly and immediately the first year we implemented the program."
-
( Kaiser Health News , an editorially independent news service, is a program of the Kaiser Family Foundation , a nonpartisan health care policy-research organization that isn't affiliated with Kaiser Permanente .)
-
---------
"Health care debate: How many actually uninsured?"
By Erica Werner, Associated Press Writer, Wednesday, August 5, 2009
WASHINGTON – It's a central goal of the president's plan: Extending health care coverage to the millions of Americans who lack it. Question is, just how many million are uninsured?
The answer could make a huge difference in the billions of dollars it will cost to remake the national system.
Barack Obama frequently cites last year's Census Bureau number of 46 million people with no health insurance. But some experts argue that figure is off by tens of millions — in one direction or the other.
The recession's continuing toll on jobs, a tendency to undercount people on Medicaid and other factors make it hard to come up with an exact number. And the most widely accepted range — 40 million to 50 million — includes some 10 million non-citizens, a detail that's generally overlooked when Obama and others talk about "uninsured Americans."
The lack of certainty about such big numbers is one more question mark for Obama and members of Congress as they try to craft a plan that would cover most of the uninsured. Obama says his goal is to cover 97 percent to 98 percent of Americans, a target that would be reached by plans taking shape in the Senate — if you don't count illegal immigrants. A bill crafted by House Democrats comes in closer to 94 percent.
All the plans would exclude illegal immigrants, who account for as much as 17 percent of the uninsured, according to the Pew Hispanic Center.
"I want to cover everybody," Obama said at a news conference last month. "Now, the truth is that unless you have a what's called a single-payer system in which everybody is automatically covered, then you're probably not going to reach every single individual."
Some people don't want health insurance or just don't bother to get it, but most people who don't have it can't afford it, Obama said.
"So I think that the basic idea should be that in this country, if you want health care, you should be able to get affordable health care," he said.
New Census Bureau figures expected next month could scramble the equation, adding billions in costs if the numbers come in higher than expected, or reducing costs if the numbers are lower.
There could be serious implications "if we all of a sudden found that instead of 45 million uninsured there are 35 million," said Michael O'Grady, a senior fellow at the University of Chicago's health policy and evaluation department and a former assistant secretary at the Department of Health and Human Services.
A lower figure could cut two ways: making Congress' job cheaper, but also making the country's health care woes seem less pressing.
Even if there are fewer uninsured than now estimated, health experts emphasize that it's still a lot of people, and being uninsured has consequences. The Institute of Medicine has found that uninsured people are more likely to succumb to illness and suffer premature death.
Still, some overhaul foes are accusing the media of overreporting the number of uninsured in order to frighten the public and "bolster calls for universal government-run insurance coverage," as a report by the conservative media watchdog Media Research Center's Business and Media Institute put it.
The 46 million number (actually 45.7 million) cited by Obama and others comes from the Census Bureau's annual Current Population Survey for 2007. It's the consensus figure, but some researchers believe the CPS overstates the number of uninsured people, partly by undercounting how many people are on Medicaid, the federal-state program for the poor.
Another government survey, the Medical Expenditure Panel Survey done by the Department of Health and Human Services, says that about 40 million people were uninsured for all of 2007, and about 70 million were uninsured for part of the year.
All those numbers are out-of-date. Taking into account the effects of the recession, with widespread job losses cutting into employer-provided health care — more than 5 million jobs have been lost since last August — researchers at the Urban Institute and elsewhere estimate that the present-day number of uninsured is closer to 50 million. That's the number used by the Congressional Budget Office.
The Census Bureau is releasing its Current Population Survey for 2008 on Sept. 10. Then, later in September, for the first time, it's releasing health coverage information collected by the American Community Survey, which has a much larger sample size than the CPS. Some researchers are expecting that number to be more precise.
___
On the Net:
U.S. Census Bureau Current Population Survey: www.census.gov/cps/
Medical Expenditure Panel Survey: www.meps.ahrq.gov/mepsweb/
---------
"Health care needs new prescription"
The Berkshire Eagle, Letters, 8/8/2009
Hospitals in Massachusetts are in trouble. Nurses are being laid off. Clinics are closing. Yet insurance companies are posting profits and talking about making care more "efficient."
Efficient and profitable for whom? Of note, I have never had an insurance company join me with a patient to help diagnose, manage or treat a disease. They have from time to time, however, told me what not to do for my patients based upon their ideas of cost savings.
Insurance companies do not practice medicine, nursing or any other kind of care. They are holding companies for money. The public entrusts them with their cash which they in turn expect to see returned in case of illness.
Unfortunately, many of these holding companies have figured out ways not to "pay off." Does this not seem like a misdirection of resources?
A public insurance option will save money in the long run. It will go a long way toward making sure that almost everyone has basic health care. It will also provide preventative services at an affordable price which will wind up saving lives and dollars over the long run. It could act as a bulwark against industry abuses in providing health care.
It is time to let someone other than the defenders of the status quo run the discussion. Sometimes the facts do carry more weight than scare tactics and angry discourse. We’ve tried it their way and it hasn’t worked. It’s time for a new therapy.
MICHAEL C. PAYNE, M.D.
Williamstown, Massachusetts
-
www.topix.net/forum/source/berkshire-eagle/T99NE58UJP7U1GKJ8
-
---------

www.boston.com/news/health/articles/2009/08/18/comparing_bills/
-
www.washingtonpost.com/wp-srv/special/nation/health/compare-health-plans-2009/?wpisrc=newsletter
-
www.washingtonpost.com/wp-srv/special/nation/health/compare-health-plans-2009/HealthcareBills.pdf
-
---------
Prescriptions: Making Sense of the Health Care Debate
"FOR MANY CONSUMERS, FEW INSURANCE CHOICES"
By Anne Underwood - http://prescriptions.blogs.nytimes.com/author/anne-underwood/
The New York Times (Online), HEALTH, Wednesday, August 19, 2009
The debate over whether the government should offer a public insurance plan is all about competition. How competitive is the private insurance market right now? It depends on where you live.
As a general rule, the larger, more densely populated states have the most choice — and even the biggest insurer controls only a minority share of the market. According to statistics from the American Medical Association, the leading insurance provider in California covers 24 percent of the population, while in New York the figure is 26 percent and in Florida, 30 percent.
But there are nine states where a single insurer covers 70 percent or more of the people. In Hawaii, one insurer covers 78 percent. In Alabama, it’s 83 percent. And in at least 17 other states one insurer covers at least half the population.
-

-
Some members of the Senate Finance Committee, which is taking a lead on health care legislation, come from states where the insurance market is highly concentrated. The Democratic chairman, Senator Max Baucus, is from Montana, where 75 percent of people are covered by one major insurer, Blue Cross Blue Shield of Montana. For Senator Charles E. Grassley, Republican of Iowa, the figure is 71 percent, by Wellmark. For Senator Olympia Snowe, Republican of Maine, it’s 78 percent, by WellPoint.
“For many Americans, the idea that they have a choice of health plans is about as mythical as unicorns,” said Jacob Hacker, professor of political science at Yale University.
-

-
But Robert Zirkelbach, a spokesman for the industry trade group, America’s Health Insurance Plans, argues that competition abounds. “In the top 40 metropolitan areas, there are eight or more health plans in every one of them,” he said.
“Both the Federal Trade Commission and the Department of Justice have reviewed this and found that health insurance plans operate in a highly competitive market,” Mr. Zirkelbach said. “Physicians’ offices contract on average with a dozen health plans.”
The choices may not appear quite so abundant to the average consumer.
If you receive coverage through your employer, you may have a selection of two or three plans offered by your company. If you work for a small employer, your choice is likely to be limited to a single plan, if that. And if you’re an individual with a pre-existing condition, the options may be closer to zero.
What’s less evident to most people is that employers, too — particularly smaller employers — face limitations in their choices. “A large employer can self-insure,” said Brad Herring, a health economist at Johns Hopkins Bloomberg School of Public Health. In other words, the employer collects the premiums and pays them out, when necessary, to cover medical claims — generally using a commercial insurer to administer the program and supply a network of doctors and hospitals, but not to financially underwrite the coverage.
“Roughly half of people with private insurance get it from a self-insured company,” Mr. Herring said.
But small businesses, which typically do not have the resources to self-insure, tend to purchase coverage through an insurer. And that often limits their options.
For one thing, insurers are regulated by states, which means only insurers that have been approved by the state’s insurance commission can sell there.
“You can’t shop across state lines,” said Jim Wordsworth, owner of a prime steakhouse, J.R’s Stockyards Inn in Tysons Corner, Va. “I can only buy insurance from companies that have the Virginia State Corporation Commission’s approval.” (Larger employers with staffers in multiple states can purchase coverage that’s exempt from state regulation.)
As chairman of the small business council of the U.S. Chamber of Commerce and a board member of the National Restaurant Association, Mr. Wordsworth has raised the issue on Capitol Hill, but has seen no move toward changing the law to open the insurance business to interstate operations.
Mr. Wordsworth is also limited in practice, if not in theory, by the expense of trying to buy a plan as a standalone business.
“A union can buy health insurance at a huge bulk discount,” he said. “A large corporation can buy at a discounted rate. A restaurant can’t. If the National Restaurant Association had access to [group rates], that would be different.”
America’s Health Insurance Plans, the industry group — which is generally known as AHIP — says on its Web site that there are nearly 1,300 insurance providers in the United States, covering more than 200 million Americans. But this number includes many plans with the same parent company, not to mention the parent companies themselves.
“When you get down to it, in many markets, it’s more like two,” said Wendell Potter, a longtime director of communications for the insurer CIGNA, who now serves as a senior fellow in health care at the Center for Media and Democracy and has become an outspoken critic of the industry.
As critics see it, part of the problem is consolidation in the insurance industry. According to the American Medical Association, there have been 400 corporate mergers among insurance providers in the last dozen years. WellPoint alone covers 34.2 million people, according to the company’s second-quarter earnings report. UnitedHealth Group covers 29.5 million, according to its second-quarter statement.
“The largest seven insurers cover more than 100 million people, a third of the market,” said Mr. Potter, who bases his figures on federal securities filings.
In a capitalist economy, the drive to consolidate should come as no surprise. “Insurance companies need to grow their earnings per share to satisfy Wall Street investors,” said Avram Goldstein, research director for Health Care for America Now, a coalition of groups favoring a health care overhaul that includes a government-run public insurance plan to compete with private insurers
The practical question is whether this consolidation is driving up the price of premiums. In a report issued at the end of May, Mr. Goldstein’s group concluded that it is.
“Premiums have risen four times faster than wages in the last nine years,” said Mr. Goldstein. “We feel that shrinking competition among insurers is a major cause of this kind of dramatic increase.”
But Mr. Zirkelbach of AHIP emphatically disagrees.
“Hospital consolidation has driven up prices,” he said. “Price Waterhouse Coopers studied this and found that in the last 20 years, benefit costs have risen 8.7 percent every year. During the same period, premiums have gone up the same amount, so there’s a correlation in the increase of premiums and the cost of the services that are provided.”
Would non-profit coops provide meaningful competition?
Mr. Potter, the former CIGNA officer, is skeptical.
“Philadelphia, my hometown, is dominated by Independence Blue Cross and Aetna,” he said. As it happens, that’s where CIGNA’s has its headquarters. “But CIGNA has a small presence there,” he said. “The market is largely locked up by the dominant companies.”
And if CIGNA can’t gain a more meaningful base in its own hometown, “a small, non-profit co-op doesn’t stand a chance,” Mr. Potter said. “It’s like a grocery store competing against Wal-Mart.”
Would a government-run public insurance plan help? Proponents say it would, by providing the competition to contain costs.
But Mr. Zirkelbach of AHIP said, “A new government-run plan would significantly disrupt the coverage that people currently rely on.”
“The important question to ask is, do individuals, families and small business have access to a variety of plans to choose from?”
At the moment, there is little consensus on the answer.
---------
"Competition lacking among private health insurers"
By Ricardo Alonso-zaldivar, Associated Press Writer, Saturday, August 22, 2009
WASHINGTON – One of the most widely accepted arguments against a government medical plan for the middle class is that it would quash competition — just what private insurers seem to be doing themselves in many parts of the U.S.
Several studies show that in lots of places, one or two companies dominate the market. Critics say monopolistic conditions drive up premiums paid by employers and individuals.
For Democrats, the answer is a public plan that would compete with private insurers. Republicans see that as a government power grab. President Barack Obama looks to be trapped in the middle of an argument that could sink his effort to overhaul the health care system.
Even lawmakers opposed to a government plan have problems with the growing clout of the big private companies.
"There is a serious problem with the lack of competition among insurers," said Republican Sen. Olympia Snowe of Maine, one of the highest-cost states. "The impact on the consumer is significant."
Wellpoint Inc. accounted for 71 percent of the Maine market, while runner-up Aetna had a 12 percent share, according to a 2008 report by the American Medical Association.
Proponents of a government plan say it could restore a competitive balance and lead to lower costs. For one thing, it wouldn't have to turn a profit.
A study by the Urban Institute public policy center estimated that a public plan could save taxpayers from $224 billion to $400 billion over 10 years by lowering the cost of proposed subsidies for the uninsured, while preserving private coverage for most people.
"Right now, there's no incentive for insurers or big hospital groups to negotiate with each other, because they can pass higher payments on through premiums," said economist Linda Blumberg, co-author of the report. "A public plan would have the leverage to set lower payment rates and get providers to participate at those rates."
"The private plans would come back to the providers and say, 'If you don't negotiate with me, you're going to be left with only the public plan.'" Blumberg continued. "Suddenly, you have a very strong economic incentive for them to negotiate."
Insurers contend their industry is extremely competitive, and a public plan is unnecessary. About 1,300 carriers operate across the country, although many only have a small share of the market in their states.
"You can have a very competitive market and still have companies with a high market share," said Alissa Fox, a top Washington lobbyist for the Blue Cross Blue Shield Association.
Fox points to the federal employee health program, which also covers members of Congress. It offers a total of more than 260 options and 10 nationwide plans. Despite all the choices, about 60 percent of federal workers pick a Blue Cross plan.
"Insurers need to be of a significant size to best serve their customers and make sure that people get the best value," Fox said.
Nonetheless, lawmakers are concerned. Big insurers are getting bigger. Small businesses in particular have fewer and fewer options for getting coverage.
Congressional investigators this year looked at insurers catering to small employers around the country. The Government Accountability Office found that the median _or midpoint — market share of largest carrier increased to 47 percent in 2008 from 33 percent in 2002.
There's widespread recognition among lawmakers that a health care overhaul should foster more competition among insurers. The debate is over how far to go.
The basic framework lawmakers are looking at would encourage competition, even without a government plan. It calls for setting up a big insurance purchasing pool called an exchange. It would be open, at least initially, to individuals and small businesses. The government would offer subsidies to make premiums more affordable.
Consumers would find it much easier to shop for a plan through the exchange. For one thing, they would be able to readily compare benefits and premiums in different plans. Also, participating insurers would have to take all applicants and not charge higher premiums to those in poor health.
Offering the option of a public plan would supercharge the competition, supporters say.
Blumberg envisions a plan that pays medical providers more than Medicare, but less than private insurance. Her study estimated it could grow to 47 million members, leaving 161 million with private insurance. Even so, that would make the new public plan one of the largest insurers in the country, rivaling Medicare, Medicaid and big private companies such as Wellpoint and UnitedHealthcare.
It's a scenario that gives pause even to traditional adversaries of the insurance companies.
"The fear and concern is that the public plan could become the market-dominant plan," said Dr. James Rohack, president of the American Medical Association. "When you've got the federal government involved, it can infuse money into a plan to keep it solvent even if the premiums are lower than its actual costs."
Snowe, among the few Republican senators still trying to come up with a bipartisan compromise, wants to hold back on creating a public plan for now and give insurers one last chance to show if they can keep costs in check.
That's doesn't go far enough for liberals, who are loath to give the insurance industry tens of millions of new customers supported by taxpayer subsidies.
"It would give the industry a windfall without any countervailing force to require them to lower their costs," said Richard Kirsch, national campaign manager for the advocacy group Health Care for America Now. "The insurance companies could continue to jack up premiums while getting a whole new market."
---------
---------
-

-
Dr. Harry J. Shriver III meets one of the patients of Group Health Cooperative of Puget Sound, one of the nation’s larger health co-ops. (Stuart Isett for The New York Times)
-
Prescriptions: Making Sense of the Health Care Debate
"SO WHAT'S A HEALTH INSURANCE CO-OP, ANYWAY?"
By Anne Underwood - http://prescriptions.blogs.nytimes.com/author/anne-underwood/
The New York Times (Online), HEALTH, August 17, 2009
If a public insurance option were to be abandoned, it could be replaced by an alternative favored by some moderates like Senator Kent Conrad, Democrat of North Dakota: the health insurance cooperative. Legislators have not spelled out how these plans might work, but health insurance co-ops do have a history in this country. Anne Underwood, a freelance writer, quizzed Timothy Stoltzfus Jost, a law professor at Washington and Lee University who has written extensively on health care policy, including the feasibility of establishing health insurance co-ops.
Q.What is a nonprofit co-op?
A.The basic idea is that consumers get together and start a company to produce something that otherwise might not be produced or would be underproduced. Co-ops are a familiar concept in the United States, especially in rural areas. I live in western Virginia, and we belong to an electric co-op that produces our power. Farm co-ops and dairy co-ops are also common.
Q.So co-ops can be formed to provide health insurance, too?
A.We had them in the 1930s and 1940s, because the Farm Security Administration sponsored them before we had health insurance. There were 600,000 people in the Midwest who were insured through them. Texas was a big area for them.
Q.What happened to them?
A.The Farm Security Administration withdrew support in 1947, and they collapsed. They had a hard time getting going anyway. Two have survived — Group Health Cooperative of Washington and Health Partners in Minnesota. From everything I’ve read about them, they function reasonably well. But they’ve basically become like other insurance companies with a few little added bells and whistles for their members.
But one thing that it’s important to get straight from the beginning is the difference between insurance co-ops and health insurance purchasing co-ops. There was a real movement in the 1990s to purchase insurance through co-ops. Those are similar to the exchanges that are being proposed. A few of them got going. They were not remarkably successfully, either. The idea was that consumers bargain with insurance companies to buy insurance. They’re not insurance providers themselves.
Q.So what we’re talking about are insurance co-ops that would function as insurers themselves.
A.The argument I make is that it’s really hard to start an insurance company. You don’t just get a bunch of people together and say, “We’re going to start an insurance co-op.” The biggest problem is coming up with a network. You have to find doctors and hospitals and negotiate contracts. Most are already locked up by the dominant insurers. They’re not going to give you — a tiny co-op — a better deal. That’s assuming they’ll deal with you at all. The alternative would be to rent a network, but you’re basically buying your product from your competitor. There’s no way you’ll get a good deal there, either.
Q.What are some of other challenges in setting up a co-op?
A.You need to establish a brand identity, figure out how to handle claims, develop actuarial expertise, establish reserves, meet state licensing requirements and solvency requirements.
Q.Does it improve competition in any way?
A.What you have in the United States now is concentration of insurance markets. You hear this stuff about 1,300 insurers in the United States and all this competition. But just try to get more than one of them to bid on your contract for a health plan in the Shenandoah, where I am. One insurer controls 87 percent of the market in Harrisonburg, Va. That’s true in many places. The idea that there are 1,300 insurers and that we have access to all of them is like saying there are 10,000 produce stands in U.S. If there’s only one within 10 miles of where you live, that’s the one you have access to.
Health insurance is very local. It’s very hard to break into an insurance market. The thought that you’ll have a few businessmen get together and set up a co-op that will compete with Aetna or Cigna is just dreaming. It’s not going to happen.
Q.So how would a public plan be superior?
A.If you had a public plan that could use Medicare rates, the infrastructure would already be there. It could use the Medicare network. Providers could always opt out, as they do today. Some doctors won’t take Medicare patients. The Energy and Commerce bill with Blue Dog amendments allows the secretary of health and human services to negotiate rates. Any provider who didn’t want to be in the public plan could opt out.
The United States government already has brand identity. It could compete. Maybe it would be a lousy competitor and fail, or maybe it would be a great competitor and force private insurers to compete and come up with a product that was more affordable than what they’re selling now. I don’t see a problem with trying it.
The idea that the public plan will dominate the market, I don’t see that. As the president said, we have a post office, Federal Express and U.P.S. I use all three. The idea [of relying solely on private insurers] is like saying we’ll abolish the post office and give people vouchers to send letters with Federal Express. That’s what we’re doing if we don’t have a public plan.
Who knows? Maybe some consumers might put together a co-op that would survive. But the idea that co-ops will provide competition in the private market that would have effect on cost is an illusion. We’re talking about using taxpayer money to pay money to private insurers without any competition. How crazy is that?
Q.So what’s the appeal?
A.It’s a co-op, a consumer-run business — not the government taking over health care. Second, the idea of a co-op is familiar in the upper Midwest. They have dairy co-ops and electrical co-ops. It’s an idea familiar to constituents, and those co-ops work reasonably well for producing certain kinds of goods in certain markets. The problem is, they don’t make sense for health insurance.
The argument that we’re headed toward government-run, socialized medicine plays pretty well in a lot of conservative parts of the United States. This is an alternative. The problem is, it’s an alternative that wouldn’t work.
Q.Would nonprofit co-ops at least help to control costs?
A.I don’t see how it does anything to control costs. I don’t see much in the legislation outside of Medicare reforms that will control costs, except for the public plan.
I also see it as a strategy to get a bill through the Senate Finance Committee. The final bill that comes out of conference may look different. I hope so.
The other thing is, nobody has seen the co-op proposal yet.
Q.Might health care co-ops be structured in different ways?
A.I did a memo on how you might structure one to work, if you established a national cooperative. If the federal government set up a co-op itself, the co-op could then be set up regionally and funded adequately to get things going. You might be able to come up with a co-op that would in fact work.
But I still think it is a poor alternative to the vigorous public plan.
Q.Should we be worried that the public plan will fare so well that we end up without private alternatives?
A.In Germany and Australia, they have competition of public plans and private plans. In fact, what has happened is that the market stabilizes, the public plan provides things some people want, and private plans provide things other people want. What you end up with eventually is a market in which people get what they want.
The Congressional Budget Office predicted in its analysis of the House bill that about two-thirds of people who had the option would go for private market and one-third for public. The vast majority — about 160 million — would stay in employer-covered plans, because the exchange wouldn’t be available to them. Probably some people will go with the public option because it’s cheaper. Others may think private insurance will offer more care or broader coverage.
The market will sort itself out, just as the market for automobiles sorts itself out. We don’t have to all buy top-end cars. In Germany, 50 percent of people go public, and 50 percent private. I think it’s unlikely the the public plan would drive private insurers out of business.
-----
"Health co-ops have checkered history"
By Associated Press, Monday, August 17, 2009, www.bostonherald.com - U.S. Politics
WASHINGTON — The Obama administration has signaled that it might accept health care cooperatives instead of a government-run health insurance program to compete with private insurers.
Interest groups disagree on whether such co-ops would have enough negotiating clout to help consumers without threatening private insurance companies. Here, in question and answer form, is a look at the issue based on interviews with several authorities, including the chief proponent of health co-ops, Sen. Kent Conrad, D-N.D.
Q: How would a health care co-op work?
A: As a nonprofit, member-owned group, it would assemble a network of health care providers and negotiate payment rates with them.
Q: How many co-ops would there be, and how many members would each have?
A: There are no set numbers. Co-ops could operate on state, regional or national levels. Conrad says each would need at least 500,000 members to succeed.
Q: How would a co-op affect me?
A: Membership would be voluntary. Consumers would decide whether a co-op’s costs, coverage, provider networks and other features are superior to those of private plans.
Q: How could a co-op offer a better alternative?
A: Co-ops presumably would reduce or eliminate some costs, including profits, to compete effectively with private insurers.
Q: Would that drive insurance companies out of business?
A: Unclear. Proponents say co-ops would force private insurers to be more efficient and fair, but the co-ops would not have enough advantages to threaten good companies.
Q: Would co-ops have enough collective bargaining power to demand good rates from providers?
A: Some experts say co-ops would need a nationwide board to negotiate such rates on behalf of all co-ops, rather than have each group bargain on its own. Others say a nationwide board is not essential. Conrad’s Senate proposal has yet to decide the matter.
Q: What is the history of health care co-ops in America?
A: Very uneven. Many have failed over the decades because they were unable to compete effectively or because tensions between doctors and consumer-oriented governing boards could not be resolved. But some, including a co-op in Washington state, have operated successfully.
Q: What would be the federal government’s role?
A: The government would provide up to $6 billion to get co-ops started. After a few years it would turn over all operations to the co-ops’ governing boards, and the co-ops would become self-sustaining. Conrad has yet to say whether co-ops should be required to repay some of the federal money.
Q: What are the biggest complaints about health care co-ops?
A: Critics on the left say they would be weaker than a government-run insurance plan and therefore unable to really compete with private insurers. Critics on the right say taxpayers and politicians might be too invested in co-ops to ever agree to eliminate the government’s role in them.
Q: Would co-ops significantly improve the nation’s health care system?
A: Perhaps. But even Conrad says other factors are more important in trying to control costs and improve quality. They include changing incentive formulas to reward providers for good outcomes rather than the quantity of procedures and tests, he says.
---------
-

-
Dr. Marcia Angell, a senior lecturer at Harvard University and former editor of The New England Journal of Medicine, in her office in January. (Jodi Hilton for The New York Times)
-
Prescriptions: Making Sense of the Health Care Debate
"Questions for Dr. Marcia Angell"
By Anne Underwood - http://prescriptions.blogs.nytimes.com/author/anne-underwood/
The New York Times (Online), HEALTH, August 12, 2009
Dr. Marcia Angell is a senior lecturer in social medicine at Harvard Medical School and former editor of The New England Journal of Medicine. A longtime critic of the pharmaceutical industry, she has called for an end to market-driven delivery of health care in the United States. She spoke with freelance writer Anne Underwood.
Q.President Obama hopes to increase the number of Americans with insurance and to rein in costs. Do you believe any of the plans under consideration by Congress will accomplish those goals?
A.They won’t, and that’s the essential problem. If you keep health care in the hands of for-profit companies, you can do one or the other — increase coverage by putting more money into the system, or control costs by decreasing coverage. But you cannot do both unless you change the basic structure of the system.
Q.Segments of the health care industry — pharmaceutical companies, for instance — are promising to cut costs.
A.It’s not going to happen. These are investor-owned companies. Their fiduciary responsibility is to maximize profits. If they behaved like charities, heads would roll in the executive suites.
Q.But what about market mechanisms for reducing costs? Wouldn’t the public option, for instance, provide competition for the insurance companies?
A.Theoretically it would, but I doubt the public plan will pass. Industry is lobbying against it, and the president has not said this is a “must.” Even if it does pass, I’m afraid the private insurance industry will use their clout in Congress — and they have enormous clout in Congress — to hobble the public option and use it as a dumping ground for the sickest while they cream off the young and healthy for themselves.
Q.How? Won’t insurance companies have to cover all applicants regardless of health status?
A.It’s hard to regulate an enormous industry without setting up a bureaucracy to oversee it. That’s very expensive and creates a whole new set of problems.
Q.How about the individual mandate? Wouldn’t it reduce costs per capita by bringing in young, healthy people who are currently uninsured?
A.No. In Massachusetts [which enacted an individual mandate in 2006], there is no real price regulation. Essentially what the mandate does is say to people, you will go into this treacherous market and buy insurance at whatever price the companies choose to charge. In effect, it’s delivering a captive market to these profit-oriented companies.
Q.Are people at least getting better health care in Massachusetts now?
A.Massachusetts already spends one-third more on health care than other states, and costs are rising at unsustainable rates. As a result, they’re chipping away at benefits, dropping beneficiaries and increasing premiums and co-payments.
Q.Then what’s the path to meaningful cost control?
A.The only way to both control costs and have universal comprehensive coverage is a single-payer system — a nonprofit, single-payer system. Nothing else will work. All other advanced countries have some form of a single-payer system, and they pay less than half as much per person as we do. We should be asking, why is that so? It’s not because we provide more basic services. We do provide more tests and procedures for those who can pay, but not more basic services — and we don’t cover everybody. So why is it so? We are the only advanced country that delivers health care in a system that’s set up to generate profits, not to provide care.
Q.If a single-payer system isn’t feasible politically, aren’t the current proposals at least better than doing nothing? Isn’t half an aspirin better than none?
A.I think not. As costs continue to soar, people will not say, “That didn’t work. Let’s try a single-payer system.” Instead, they’ll try to pay for the costs in piecemeal ways, by increasing co-pays and deductibles, by limiting services, by making the system less equitable and less comprehensive. I’m afraid the lesson they’ll draw is that universal care is impossible.
But I’m not convinced that getting a single-payer system now is politically infeasible. The public would be happy with Medicare for all. Polls have shown that the public loves Medicare. The problem isn’t the public. It’s Congress, which caves in to special interests.
Q.If Congress is reluctant to cut out the insurance companies, is that partly because they, like the major banks, are too big to fail?
A.A nonprofit, single-payer system would lead to job losses in this sector, which constitutes 17 percent of the economy. But what about the other 83 percent of the economy? They’re being bled to death. Businesses can’t compete globally because the cost of providing coverage to their workers is so exorbitant. Whatever loss of jobs you might see would be more than offset by benefits and job gains in the rest of the economy.
[As for the insurance companies,] you could introduce the program incrementally. You could do it state by state. Or probably better, you could do it decade by decade. Medicare kicks in at age 65. In the first stage, you could take it down to 55. Between 55 and 65, people are vulnerable. They’re losing jobs, losing health care. They’re starting to have more medical needs. After a few years, you could drop it to 45, then 35. It would give insurance companies time to adjust.
Q.But Medicare is already hugely expensive. How can we afford such a plan for everyone?
A.Medicare costs are rising at an unsustainable rate because care is provided in a profit-maximizing system. The prescription drug benefit was nothing but a bonanza for the pharmaceutical industry. I would change that. I would also adjust the fee schedule, which preferentially rewards highly paid specialists for very expensive tests and procedures. For the system to work, it would have to be a nonprofit delivery system.
Q.How much could we save in administrative costs?
A.On average, the private insurance industry takes 15 to 20 percent right off the top of the premium dollar for its administrative costs and profits. That’s a lot to siphon off by an industry that adds almost nothing of value. It’s just a middleman. Medicare has overhead costs of less than 3 percent.
With the money in the system right now, we could cover everyone for every medically necessary service. But the system has to be distributed according to medical need and not as it currently is — as a commodity. Today, those who can pay get lots of M.R.I.’s they don’t need, while those who are uninsured can go without ones they do need.
Q.Military historians say we’re always fighting the last war. Is Mr. Obama now fighting the last health care war, in which Congress rejected the Clinton plan partly because it was developed without consulting other interested parties?
A.Yes. Mr. Obama has decided that he will listen to everybody. But it’s not working for him, because the public can’t become enthusiastic about a plan that doesn’t exist. That’s what he’s asking. Now Congress has gone home, and for the next month the special interests will be out there scaring people with stories of rationing and socialized medicine.
Q.Is the president really bringing everyone to the table?
A.He’s bringing everyone to the table except the single-payer people. It’s very odd. When he was a state senator, he emphatically favored a single-payer system. And in his July 22 press conference on health care, he stated that the only way to provide universal health care is with a single-payer system. Then he moved right on, as if that was somehow self-evidently absurd.
Q.So are you opposing this reform?
A.I am, though not for the same reasons as the Republicans and Blue Dogs. I’m opposing it more in sorrow than in anger. I’m afraid the president squandered a good opportunity.
---------
8/19/2009
-
Health Care
-

-
Graphic shows health care expenditures as a percentage of GDP.
-

-
Chart shows the results of a Gallup poll on opinions on healthcare reform.
-

-
Chart shows life expectancy change, 1975 to ...
---------
-

-
---------
"It's not all or nothing"
By Charles Joffe-Halpern, Op-Ed, The Berkshire Eagle, Thursday, August 20, 2009
NORTH ADAMS, Massachusetts
If some form of national health care legislation is going to be passed this year, it would be wise to pay attention to Harvard sociologist Theda Skocpol's observations in her analysis of the failed Clinton health care initiative of 1993-94, "Boomerang -- Health Care Reform and the Turn Against the Government."
Skocpol observes that in post-Vietnam era politics: "The proliferation of...advocacy and interest organizations in U.S. politics has outflanked or internally divided the political parties, especially the Democratic Party." She added that "Democrats and the cacophonous array of advocacy groups and interests swirling around them never did unite around any...compromise approach to comprehensive health reform."
There is real danger this may repeated now, as seen in the response to President Obama indicating that he may consider dropping a public option plan in any proposed health legislation. The immediate response of some is to say they won't support any health care legislation without a public plan, claiming any bill without one is not worth passing. But recently Ezra Klein, writing for the Washington Post, made important observations about a public plan:
"The public option is limited to the Americans who buy into the Health Insurance Exchanges, and the exchanges are in turn limited to the unemployed, the self-employed and small businesses.....the Congressional Budget Office estimates that 27 million Americans would be in the exchanges by 2019."
That's not nothing, but it's not much. Imagine half choose the public option (CBO estimates many fewer than that). You now have 13.5 million Americans in a public insurer with no substantive advantages over private insurance. Klein adds further that the public option is not now, and has not ever been the core of the argument for health reform, but it is now the core of the fight in Washington.
Many progressives have drawn a line in the sand around the public plan as if it is the holy grail of health reform. Klein points out, while it may be a valuable health policy experiment, it is certainly not worth abandoning health reform if we can't get it in included the final piece of legislation.
We now have an all too rare window of opportunity to pass health reform, which includes the long overdue regulation of the insurance industry and helping millions of uninsured Americans have access to health coverage. Accomplishing this will involve making compromises; that is how the political process works. As Skocpol points out though, compromising has become anathema in the post Woodstock era. Somehow we have developed the belief that if we don't get it "perfect" immediately then it's not worth doing.
It is important to realize that no piece of legislation is ever finished when it is finished. Important national programs, including Social Security, Medicare, and Medicaid have all been adjusted since they were first passed. They were enacted with the understanding that changes would need to be made over time.
In the pursuit of perfection, we may lose yet another opportunity to address some of the most vexing health care challenges facing our country, and the one's who will laugh the loudest are those who want to maintain the status quo.
-
Charles Joffe-Halpern is the executive director of Ecu-Heath Care and the president of the Board of Directors of Health Care for All in Boston. The views expressed here are his own. He can be contacted at cjoffehalpern@nbhealth.org.
-
---------
"The Uninsured"
The New York Times - Editorial - August 23, 2009
One of the major goals of health care reform is to cover the vast numbers of uninsured. But how vast, really, is that pool of people? Who are they? And how important is it to cover all or most of them?
Critics play down the seriousness of the problem by pointing out that the ranks of the uninsured include many people who have chosen to forgo coverage or are only temporarily uninsured: workers who could afford to pay but decline their employers’ coverage; the self-employed who choose not to pay for more expensive individual coverage; healthy young people who prefer not to buy insurance they may never need; people who are changing jobs; poor people who are eligible for Medicaid but have failed to enroll. And then there are the illegal immigrants, a favorite target of critics.
All that is true, to some degree. But the implication — that lack of insurance is no big deal and surely not worth spending a trillion dollars to fix — is not.
No matter how you slice the numbers, there are tens of millions of people without insurance, often for extended periods, and there is good evidence that lack of insurance is harmful to their health.
Scores of well-designed studies have shown that uninsured people are more likely than insured people to die prematurely, to have their cancers diagnosed too late, or to die from heart failure, a heart attack, a stroke or a severe injury. The Institute of Medicine estimated in 2004 that perhaps 18,000 deaths a year among adults could be attributed to lack of insurance.
The oft-voiced suggestion that the uninsured can always go to an emergency room also badly misunderstands what is happening. By the time they do go, many of these people are much sicker than they would have been had insurance given them access to routine and preventive care. Emergency rooms are costly, and if uninsured patients cannot pay for their care, the hospital or the government ends up footing the bill.
•
So how many uninsured people are out there, facing those risks? The most frequently cited estimate, 45.7 million in 2007, comes from an annual census survey. That number was down slightly from the year before, but given the financial crisis, it is almost certainly rising again.
Some or even many of those people may have only temporarily lost or given up coverage, but even that exposes them to medical and financial risk. And many millions go without insurance for extended periods.
The Agency for Healthcare Research and Quality in the Department of Health and Human Services estimates that 28 million people were uninsured for all of 2005 and 2006 and that 18.5 million of them were uninsured for at least four straight years. That does not sound like a “temporary” problem, and the picture today is almost certainly bleaker.
Various analyses have tried to decipher just who the uninsured are. These are the main conclusions, with the caveat that there is overlap in these numbers:
THE WORKING POOR The Kaiser Family Foundation estimates that about two-thirds of the uninsured — 30 million people — earn less than twice the poverty level, or about $44,000 for a family of four. It also estimates that more than 80 percent of the uninsured come from families with full-time or part-time workers. They often cannot get coverage at work or find it too expensive to buy. They surely deserve a helping hand.
THE BETTER OFF About nine million uninsured people, according to census data, come from households with incomes of $75,000 or more. Critics say that is plenty of money for them to buy their own insurance. But many of these people live in “households” that are groups of low-wage roommates or extended families living together. Their combined incomes may reach $75,000, but they cannot pool their resources to buy an insurance policy to cover the whole group.
Still, about 4.7 million uninsured people live in families that earn four times the poverty level — or $88,000 for a family of four — the dividing line that many experts use to define who can afford to buy their own insurance.
Those people who could afford coverage but choose not to buy it ought to be compelled to join the system to lessen the possibility that a serious accident or illness might turn them into charity cases and to help subsidize the coverage of poorer and sicker Americans.
YOUNG ADULTS Some 13 million young adults between the ages of 19 and 29 lack coverage. These are not, for the most part, healthy young professionals making a sensible decision to pay their own minimal medical bills rather than buy insurance that they are unlikely to need. The Kaiser foundation estimates that only 10 percent are college graduates, and only 5 percent have incomes above $60,000 a year, while half have family incomes below $16,000 a year. Many of these younger people would be helped by reform bills that would provide subsidized coverage for the poor and an exchange where individuals can buy cheaper insurance than is now available.
ALREADY ELIGIBLE Some 11 million of the poorest people, mostly low-income children and their parents, are thought to be eligible for public insurance programs but have failed to enroll, either because they do not know they are eligible or are intimidated by the application process. When such people arrive at an emergency room, they are usually enrolled in Medicaid, but meanwhile they have lost out on routine care that could have kept them out of the emergency room. They will presumably be scooped up by the mandate under reform bills that everyone obtain health insurance.
THE UNDERINSURED The Commonwealth Fund estimates that 25 million Americans who had health insurance in 2007 had woefully inadequate policies with high deductibles and restrictions that stuck them with large amounts of uncovered expenses. Many postponed needed treatments or went into debt to pay medical bills.
NON-CITIZENS Some 9.7 million of the uninsured are not citizens; of those, more than six million may be illegal immigrants, according to informed estimates. None of the pending bills would cover them.
If nothing is done to slow current trends, the number of people in this country without insurance or with inadequate coverage will continue to spiral upward. That would be a personal tragedy for many and a moral disgrace for the nation. It is also by no means cost-free. Any nation as rich as ours ought to guarantee health coverage for all of its residents.
---------
"Health care claim costs expected to rise 10.5 pct"
By Tom Murphy, AP Business Writer, August 25, 2009
INDIANAPOLIS --Costs for employer-provided health plans are expected to rise more than 10 percent within the next 12 months, a jump workers may feel in their paychecks or through changes to their insurance coverage.
An aging population, rising costs and growing patient demand for services are among the reasons for the higher costs cited in an Aon Consulting report released Tuesday.
Aon Consulting, a subsidiary of Chicago-based Aon Corp., surveyed about 60 health insurers around the country earlier this year. The study found that, on average, insurers expect to pay out 10.5 percent more in claims costs in the next year -- slightly less than the 10.6 percent increase forecast last year.
The expected increase doesn't necessarily mean the premiums employees pay will grow at the same clip. Actual increases for each insurer or plan can vary by such factors as plan design, geography or the general health of the people covered.
Some employers also might swallow the higher costs because workers this year already have had to contend with salary freezes, reductions and layoffs, said Tom Lerche, Aon Consulting's health care practice leader.
"There's one school of thought that says, 'Our employees have borne enough, let's minimize or not pass any costs along to the employee,'" he said.
However, others may ask workers to pay more through increased deductibles or copayments. They could make changes to the plans they offer, such as eliminating a traditional plan and offering a consumer-directed, high-deductible plan instead.
Lerche said most employers will consider it "an absolute business imperative" to lower any cost increases to mid- to low-single digit percentages.
Companies also could deal with rising health care costs by limiting pay increases, said Joseph Antos, an economist with the Washington, D.C.-based American Enterprise Institute for Public Policy Research. He was not involved with the Aon study.
"Employer contributions are not gifts, they're part of total compensation," he said. "And if you end up having a more expensive health benefit that your employer pays most of, that means that your wages aren't going to up as fast as they would have."
The Aon survey also found that prescription drug costs are expected to rise 9.3 percent, a slight dip from the 9.4 percent trend forecast a year ago.
Lerche said a number of brand-name drugs have lost patent protection, which allows patients to buy less-expensive generics. Employers also have encouraged their workers to use generic drugs and cost-management programs.
The health care overhaul debate currently taking place in Washington, D.C., won't control this growth. The debate's outcome and the potential savings achieved through any overhaul are both big unknowns.
In any case, the impact from any reform push likely won't be felt for a couple years, notes Antos.
"None of it will affect workers next year," he said.
Aon conducts its survey twice a year to give clients a sense of cost increases they may face as they consider benefit plan renewals. Many employers conduct open enrollment in the fall for coverage that starts the next year.
---------
"U.S. health reform estimates need long view: study"
By Susan Heavey, Tuesday, September 1, 2009
WASHINGTON (Reuters) – The Congressional Budget Office may be missing potential savings from various health reform proposals by not looking at efforts to manage or prevent expensive, chronic conditions such as diabetes and heart disease, researchers said in a study released on Tuesday.
The study, published in the Tuesday edition of the Health Affairs journal, comes as members of the U.S. Congress prepare to return to Washington next week and again take up legislation to revamp the U.S. healthcare system.
President Barack Obama has made the overhaul a top priority this year, but debate has swelled in both parties in part over the CBO's early projections the Democratic plan could cost nearly $1 trillion.
Obama and other Democrats have argued the CBO does not factor in how improvements to care such as primary doctor visits, although costly at first, could improve people's health and lower costs over time.
The nonpartisan CBO, charged by Congress to estimate the cost of various programs, now uses a 10-year forecast that cannot look at the cost of programs aimed at diseases that can last for decades, researchers at the University of Chicago said.
Instead, the CBO should use methods that would weigh savings from earlier treatment and other intervention that could help reduce costly complications from conditions that arise when left untreated or improperly treated, they said.
Lawmakers need cost estimates that look at a period of 25 years for healthcare legislation, they said in their study, which was sponsored by diabetes drug maker Novo Nordisk A/S and looked at a scientific model to help estimate such costs for long-term diseases.
"Although this would not be necessary for the vast majority of cost estimates produced by the CBO, it would improve the information available when Congress considers health legislation with implications for the treatment of a relatively small number of costly chronic illnesses," they wrote.
In the study, researchers at the University of Chicago's National Opinion Research Center said new longer-term estimates would also help legislators and others estimate how having healthier, longer-living patients would affect costs.
In their model, the researchers used the example of diabetes, which affects nearly 8 percent of the U.S. population, or 24 million Americans, and factored in the costs of complications such as blindness, kidney failure and stroke.
They projected the disease would cost $336 billion a year 25 years from now. They then factored in the costs of prevention programs that would include medication and routine testing and how they could save money over time.
While such methods would need to be adjusted as treatments change, it could provide the CBO a starting point to look more long term, they said.
(Reporting by Susan Heavey; Editing by Peter Cooney)
---------
"Census: Uninsured rises to 46.3 million"
By Hope Yen, Associated Press Writer, September 10, 2009
WASHINGTON – The number of Americans without health insurance rose to 46.3 million last year as people began losing jobs and coverage in the current recession. The poverty rate hit 13.2 percent, an 11-year high.
The Census Bureau's annual report released Thursday offers a snapshot of the economic well-being of American households for 2008, the first full year of the recession. It comes as Congress engages in its high-stakes debate over a health care overhaul, following a renewed plea Wednesday night by President Barack Obama to pass sweeping legislation.
Analysts cautioned the numbers for 2008 could significantly understate today's reality since they do not capture the economic impact in the first half of 2009, when unemployment was steadily rising. The census also asked people whether they had health coverage anytime during 2008, and thus may not include those who lost jobs and their insurance after the financial meltdown last fall.
The jump in poverty could add a new dimension to the health care debate, since eligibility for government aid programs such as Medicaid and children's insurance is tied to the federal poverty level. That means more people will qualify, potentially adding strain to states already struggling to balance budgets due to the recession.
Speaking at the White House, Obama acknowledged that the number of those without coverage may be higher than the Census figures.
"The situation's grown worse over the last 12 months," he said. "It's estimated that the ranks of the uninsured have swelled by at least 6 million."
The figures show about 46.3 million people were uninsured last year. That's higher than the 45.7 million in 2007, due to the steady erosion of employer-provided health insurance. Still, the level remained just below the peak of 47 million who were uninsured in 2006, because of the growth of government insurance programs such as Medicaid for the poor.
The percentage of Americans without health coverage rose to 15.4 percent, which is not statistically different from 15.3 percent in 2007.
Texas had the highest share of people who were uninsured, at about 1 in 4 residents, according to rough calculations by the Census Bureau. It was followed by New Mexico, Florida, Louisiana and Alaska. On the other end of the scale, Massachusetts — which has a mandatory health insurance law — had the lowest share, at 5.5 percent.
The nation's poverty rate increased to 13.2 percent, up from the 12.5 percent in 2007. That meant there were 39.8 million, or nearly 1 in 7 people, living in poverty in 2008, an increase of about 2.5 million from the previous year. It was the highest level since 1997, when the rate stood at 13.3 percent.
The official poverty level is now $22,025 for a family of four, based on a calculation that includes only cash income before deductions for taxes. It excludes capital gains or accumulated wealth; it also does not factor in noncash government aid such as food stamps or tax credits.
The median — or midpoint — household income declined to $50,303.
In terms of the uninsured, the Census data show employment-based health insurance declined from 177.4 million to 176.3 million, driving the overall decreases in insurance. In contrast, the number covered by government health insurance such as Medicaid and S-CHIP climbed from 83.0 million to 87.4 million. Children, in particular, saw improvement, helped by recent expansions of government health insurance.
Among the findings:
_The number of uninsured children declined from 8.1 million, or 11.0 percent, in 2007, to 7.3 million, or 9.9 percent, in 2008. Both the rate and number of uninsured children are the lowest since 1987, the first year that comparable health insurance data were collected.
_The number of uninsured among whites increased to 10.8 percent, or 21.3 million, up from 10.4 percent, or 20.5 million, in 2007. Blacks, meanwhile, were not statistically different from 2007, at 19.1 percent and 7.3 million. The uninsured rate for Asians in 2008 rose to 17.6 percent, up from 16.8 percent.
_The percentage of uninsured Hispanics decreased to 30.7 percent in 2008, from 32.1 percent in 2007. The number of uninsured Hispanics was not statistically different in 2008, at 14.6 million.
_Divided by region, the uninsured were mostly likely to be found in the West (17.4 percent) and the South (18.2 percent). That is in contrast to 11.6 percent for the Northeast and the Midwest.
The increases in the uninsured were likely to be just the beginning. Based on current job losses, some researchers estimate the present-day number of uninsured is closer to 50 million, the number now used by the Congressional Budget Office.
Diane Rowland, executive vice president of the Kaiser Family Foundation, also noted the decreases in the percentage of people with employer-provided insurance in 2008 for the eighth year in a row. She cited the proliferation of small businesses, which typically decline to offer insurance because of rising premium costs, which could lead to additional declines in private insurance even if the economy improves.
---------
"Politics trumps policy in health debate"
Brown Patrick O'connor, Carrie Budoff Brown, POLITICO, September 14, 2009
The left-vs.-right battles that dominate American politics — and that President Barack Obama has sought desperately to avoid — are about to move center stage in the health care debate.
After months of discussion about once-obscure policy particulars, the debate is reverting to well-trod political terrain over issues that have long divided Democrats and Republicans: whether lawsuits against doctors should be capped, how much care to provide the poor, whether to pay for abortions and whether people who came here illegally should be covered.
The emergence of these now-familiar dividing lines doesn’t bode well for a White House — and a president — that has been eager to avoid the politics of the past and already has had enough trouble selling the idea of reform in broad strokes. In his speech to Congress last week, Obama tried to assuage concerns about abortion and illegal immigration and offered to include new restrictions on medical malpractice lawsuits, extending an olive branch to Republicans that only seemed to reignite a long-standing debate.
The Senate Finance Committee, which is expected to produce a bill this week, has been immersed in discussions on these hot-button issues over the past week as Chairman Max Baucus tries to reach an agreement with a group of two fellow Democrats and three Republicans.
And these fights could very well overshadow debate on matters of health care policy as the rank and file start making more noise about them. Obama himself might also have to wade into the debate once the inevitable deadlocks emerge.
“Most of this stems from the way the president talks about reforming health care,” said Michael Cannon, director of health policy studies at the Cato Institute. “The administration has been trying too hard to project an air of inevitability without getting into specifics.”
Here are the coming flash points:
Medicaid
A proposed increase in this program to provide medical coverage to the poor barely garnered any notice over the summer, when House Democrats approved a $438 billion expansion of Medicaid. Democrats want to raise the threshold for receiving Medicaid to 133 percent of the poverty level.
But it’s not escaping notice any longer. This fight is one that could be waged between the chambers — and with state governments, who pay for part of the coverage. House lawmakers wanted to use federal money to fund the expansion.
Senate negotiators want the states to bear part of the burden in order to reduce the overall costs of the federal tab — an idea that is, not surprisingly, pretty unpopular back in the statehouses, most of which have budgets deep in red ink.
But the fight could go deeper. It could reignite ideological concerns from Republicans and small-government Democrats who have problems with federally funded health care programs — even one with as long a history as Medicaid. And conservative groups will only add more fuel to the fire.
“The federal government shouldn’t be expanding Medicaid. It should be cutting it,” said Cannon.
Baucus said Monday he hopes the final Senate Finance Committee bill will actually be less difficult for states to shoulder than many states originally feared. But that doesn’t mean it won’t be controversial, even within the Finance Committee, where Sen. Olympia Snowe, the Maine Republican who is one of only three Republicans still at the table, has raised concerns about putting too much burden on the states.
Illegal immigration
South Carolina Rep. Joe Wilson, a genial back-bencher, earned national scorn (and acclaim, in some circles) for calling Obama a liar after the president claimed his health care bill won’t offer any benefits to illegal immigrants.
The now-infamous episode, for which Wilson apologized, renewed a debate that stirs as much angry opposition as any in American politics — making it such a powerful foil for Republicans and other critics of health care reform.
Democrats in the House went out of their way to include a passage in their bill to explicitly bar illegal immigrants from receiving any health care benefits established in the bill.
However, there are pre-existing loopholes that make it difficult to prevent illegal immigrants from receiving emergency-room treatment under Medicaid, and the Congressional Research Service acknowledged that some could share in subsidies to purchase insurance if others in their household already qualify.
The Senate Finance Committee is looking to create a verification system that would bar illegal immigrants from receiving any benefits under these programs. The bipartisan group of six senators is also weighing a five-year delay on benefits for legal immigrants, which Sen. Chuck Grassley (R-Iowa) favors.
The White House position is that illegal immigrants would be barred from buying insurance in the exchange, and the verification system could mirror one currently used for government entitlement programs. Legal immigrants should be able to participate in the exchange, according to the White House.
But immigrant advocates complain that these political arguments miss the point on immigration and health care. “The Senate Republicans and Democrats, the Gang of Six, are just folding in the face of one heckler,” said Ali Noorani, executive director of the National Immigration Forum, an advocacy group for immigrants.
Ira Mehlman, spokesman for the Federation for American Immigration Reform, said the prohibition on illegal immigrants must apply to the exchange and any sort of public option, and the Senate Finance Committee bill should stipulate a verification system.
Medical malpractice reform
Obama appeared to throw Republicans a bone last week when he acknowledged that “defensive medicine may be contributing to unnecessary costs.” He even directed his administration to explore pilot programs to limit unnecessary lawsuits against doctors.
The Senate Gang of Six received legislative language Monday from staff on providing federal funding to the states to experiment with medical malpractice reform programs.
The GOP has been asking the president for months to include some form of malpractice reform in the health care reform bill. But most Republicans were skeptical in the wake of his speech.
The fight typically splits over whether to cap the money a jury can award plaintiffs in a medical malpractice lawsuit. Until he offers more details, or until congressional negotiators reach some agreement, Republicans will continue to view his offer as a rhetorical flourish meant to win more points with voters than corral GOP votes.
“While his demonstration program might be a step in the right direction, the devil is in the details,” said Lisa Rickard, president of the U.S. Chamber Institute for Legal Reform.
Abortion
In his speech to Congress, Obama said “no federal dollars will be used to fund abortions,” sparking another round of head-scratching about whether the legislation will actually allow federal funding for abortion.
Rep. Lois Capps (D-Calif.) tried to craft an amendment in the House Energy and Commerce Committee that would allow lawmakers to keep the current ban in place without reigniting a bitter fight over abortion rights.
The current law bans federal funds from being spent on abortions, but under the Capps amendment, private insurers that already provide coverage for abortion would still be allowed to offer those services. Her amendment requires every exchange to include at least one plan that offers abortion coverage and at least one that does not.
Reproductive rights groups are fighting hard to at least preserve the Capps amendment.
“At a very minimum, there should not be backsliding for American women for their access to abortion,” said Nancy Northup, president of the Center for Reproductive Rights, who wants the Senate to match the language in the Capps amendement.
On the president’s speech last week: “The rhetoric has been unhelpful.”
Joy Yearout, communications director for the Susan B. Anthony List, a group that opposes abortion rights, said the opponents of abortion are looking for an explicit exclusion of taxpayer funds for abortion. “No matter how many times the president says abortion coverage will not be in the bill, there is no bill, and there is no language. Until we see the language, we can’t assess what it says.”
---------
"To fix U.S. healthcare, focus on value, experts say"
By Julie Steenhuysen, September 23, 2009
CHICAGO (Reuters) – The secret to fixing healthcare in the United States is to focus on value, a measure that takes into account both quality and cost, says Dr. Denis Cortese, president of the Mayo Clinic.
The Rochester, Minnesota-based network of clinics is being held up by President Barack Obama and health policy experts as a potential model for healthcare reform, in part because it offers good care at a fair price.
In a commentary on Wednesday in the New England Journal of Medicine, Cortese says under the U.S. healthcare system the country spends more than any other but the results are uneven at best.
Costs vary drastically, with some centers spending $10,000 on tests to arrive at a diagnosis, while others may spend $15,000 to get to the same result.
To get healthcare moving in the right direction, Cortese argues for using currently available measurements to devise a "value score" that takes into account patient satisfaction, safety, cost and outcomes -- Did the patient get better?
"We could thus create a value score for each medical institution and make it publicly available," Cortese and colleague Jeffrey Korsmo wrote.
Armed with that information, patients could choose hospitals that represent the best value, forcing doctors and caregivers to compete on cost, service, safety and results.
Those with poor track records would lose out among healthcare value shoppers.
They also said care among different medical and surgical specialists should be coordinated, giving patients access to teams of doctors who share the same electronic medical records.
And to remove the temptation to order too many tests or procedures, they think doctors should be paid a salary -- something that distinguishes Mayo.
"The goal is to reduce conflict of interest," they wrote. "Instead, they can focus on providing the right level of coordinated care for each patient -- no more and no less."
Doctors should be offered a bonus when patients are happy with their care, they said.
Cortese and Korsmo said lawmakers looking to reform healthcare should be willing to pay for high-quality, low-cost care instead of making across-the-board cuts to Medicare, the government health program for the elderly.
GROUP PRACTICE
In a separate commentary, Dr. Francis Crosson of Kaiser Permanente in California said fixing healthcare will require a change in the way physicians are paid to foster the formation of group practices, such as Kaiser, Mayo, and Geisinger Health System in Pennsylvania.
Crosson favors payment up front for care. That way, "the physician is generally not in a position where they have to say, 'If I don't do this, I don't make that money,'" Crosson said in a telephone interview.
Instead, like the Mayo model, Crosson said doctors should be paid a salary, with modest incentives for good quality work. And physician groups should work together with hospitals in a partnership.
The result, he said, is doctors get to focus on patients.
"The quiet secret is that we have an environment in these group practices where physicians love to practice medicine. They are not telling their children, 'don't go into medicine,'" Crosson said.
(Editing by Maggie Fox and Vicki Allen)
---------
"How health care overhaul could change Medicare"
By Carla K. Johnson, Ap Medical Writer, October 2, 2009
CHICAGO – Businessman Stewart Grill, 75, believes there's waste in Medicare. He's just skeptical Congress can find and eliminate it without touching what he likes about his government health care plan.
"The talk of potential savings is a little beyond comprehension," Grill said. "Why hasn't it been saved before? It's virtually impossible to save $500 billion and not do any cutting of benefits."
The congressional plans for health care overhaul could mean a major restructuring of Medicare. Dozens of changes are being proposed in hopes of transforming the program from one that rewards doctors for each procedure they do into one that improves people's health and keeps them out of the hospital.
The changes should save money. What many seniors, including Grill, want to know is this: Can lawmakers pull this off without cutting benefits?
Like most seniors, Grill has his Medicare premium deducted from his Social Security check. He sees it as a good deal, but he's worried about Medicare's future.
His knee doctor no longer takes Medicare patients. And he has to pay two other doctors directly and wait for Medicare to reimburse him. He sees those doctors' policies as warnings that Medicare's reliability may be growing shakier.
A lifelong independent politically, Grill said he knows that slowing the rate of growth in Medicare can keep it solvent longer. He thinks that's good for him, and good for his children and grandchildren.
"The figures are so large and so hard to comprehend," Grill said. "The biggest overall problem I see is nobody wants their own ox gored."
Here's a look at the proposals and how they might affect him and other seniors:
_Medicare Advantage
More than 10 million seniors — nearly 1 in 4 — are covered by Medicare Advantage, an alternative that pays for-profit insurance companies to run their own versions of the government program. But the government is spending 14 percent more per patient in Medicare Advantage, so Congress wants to cut some of that — up to $160 billion over 10 years.
That means seniors covered by the plans may lose extra benefits like hearing aids and health club memberships. Some commercial insurers may pull out of Medicare Advantage, forcing some seniors to switch plans.
"There's no way to sugarcoat it and say there's no harm here," said Dr. Robert Berenson, a Medicare official during the Clinton administration and a senior fellow at the Urban Institute.
Everyone in Medicare pays $3 a month extra to subsidize the Medicare Advantage plans, the Leadership Council of Aging Organizations estimates.
Berenson tells seniors in Medicare Advantage it's a matter of fairness: "You've been getting extra benefits for many years beyond what the program really promised you."
_Preventing illness
Free preventive services would be more common in Medicare under the congressional plans. Medicare would pay 100 percent for mammograms, diabetes classes and other preventive services. The Senate bill would include a free annual wellness exam too.
"It starts to change the nature of the relationship from one where you go to the doctor when you're feeling sick to one that's more focused on proactive prevention," said Ken Thorpe, executive director of the Partnership to Fight Chronic Disease.
Paying doctors fairly sharpens the focus on prevention. Democrats in the House and Senate want to delay scheduled decreases in doctors' fees and provide bonus payments that would make it more lucrative to see Medicare patients.
_Staying out of the hospital
Nearly one in five Medicare patients lands back in the hospital within a month of getting out, costing billions annually.
To attack the problem, social workers in Chicago telephone patients after they leave Rush University Medical Center. The social workers find out what patients need to avoid repeat hospital trips. They help arrange rides to doctors and make sure seniors can afford their medicine.
"It can be one call or 30 calls," said Robyn Golden, who directs the hospital's older adult programs. "We call the providers to make sure they're following through when the patient says they're not."
Congress wants more hospitals to think like this. The leading Senate legislation would penalize hospitals with the highest readmission rates by reducing Medicare payments for repeat visits that could have been avoided.
_Coordinating care
A recent study found the typical primary care doctor must coordinate their Medicare patients' care with hundreds of other doctors. But rarely does any one doctor take charge of one patient's care from start to finish of a health problem.
"As it is now, the doctor asks the patient, 'What did the specialist say?'" said Joseph Baker of the nonprofit Medicare Rights Center.
Proposals in the House and Senate would set up pilot programs to better coordinate care with the goals of saving money and improving quality. Buzzwords are "medical homes" and "accountable care organizations," but the goals are the same, Baker said, "a more seamless provision of care without the bumps or gaps people experience now."
_Filling prescription drug gap
When Congress created the Medicare drug program it left a coverage gap called the "doughnut hole." More than 3 million Medicare beneficiaries a year hit this gap and start paying the full cost of their drugs until they qualify for catastrophic coverage.
Drug companies have promised a 50 percent discount on brand-name prescriptions for people in the doughnut hole. House Democrats want to eliminate the gap entirely by 2023.
___
On the Net:
Leadership Council of Aging Organizations: www.lcao.org
Medicare Rights Center: www.medicarerights.org
Partnership to Fight Chronic Disease: www.fightchronicdisease.org
---------
"Lack of health care killed 2,266 US veterans last year: study"
November 11, 2009
WASHINGTON (AFP) – The number of US veterans who died in 2008 because they lacked health insurance was 14 times higher than the US military death toll in Afghanistan that year, according to a new study.
The analysis produced by two Harvard medical researchers estimates that 2,266 US military veterans under the age of 65 died in 2008 because they lacked health coverage and had reduced access to medical care.
That figure is more than 14 times higher than the 155 US troop deaths in Afghanistan in 2008, the study says.
Released as the United States commemorates fallen soldiers on Veterans Day, the study warns that even health care provided by the Veterans Health Administration (VA) leaves many veterans without coverage.
The analysis uses census data to isolate the number of US veterans who lack both private health coverage and care offered by the VA.
"That's a group that's about 1.5 million people," said David Himmelstein, an associate professor of medicine at Harvard Medical School and co-founder of Physicians for a National Health Program who co-authored the study.
Himmelstein and co-author Stephanie Woolhandler, also a Harvard medical professor, overlaid that figure with another study examining the mortality rate associated with lack of health insurance.
"The uninsured have about a 40 percent higher risk of dying each year than otherwise comparable insured individuals," Himmelstein told AFP.
"Putting that all together you get an estimate of almost 2,300 -- 2,266 veterans who die each year from lack of health insurance."
Only some US veterans have access to medical care through the VA and coverage is apportioned on the basis of eight "priority groups."
"They range from things like people who were prisoners of war, who have coverage for life, or who have battle injuries and therefore have coverage for their injuries for life," said Himmelstein.
Veterans who fall below an income threshold that is determined on a county-by-county basis can qualify for care, but many veterans are "working poor" and fall just above the bracket.
"The priority eight group, the lowest priority, are veterans above the very poor group who have no other reason to be eligible and that group is essentially shut out of the VA," according to Himmelstein.
The study comes as the US Senate weighs health care reform legislation and whether to offer government health insurance.
Himmelstein warns that congressional proposals could still leave veterans uncovered and favors a national health care program similar to those in Britain and Canada.
---------
"Health overhaul: Understanding the pros and cons"
RICARDO ALONSO-ZALDIVAR, The Associated Press, 11/28/2009
(AP) — WASHINGTON - Maybe you've been reading the health care bill in your spare time. Then perhaps you can answer this question:
If Congress makes history and puts a bill on President Barack Obama's desk by Christmas, how long before the uninsured get medical coverage?
If you said three years or more, you'd be right. Yet many people don't realize that to keep costs down, lawmakers made compromises that might not appeal to consumers.
"There's going to be a long period of great expectations and very modest deliveries," said economist Robert Reischauer, president of the Urban Institute public policy center. That's assuming Democrats prevail.
Some questions and answers on the House-passed bill and the version the Senate will begin debating in the week ahead; both measures were written by Democrats:
Q: How many people would be covered?
A: The Senate bill would cover 94 percent of eligible Americans under age 65; under the House bill, it's 96 percent.
That's a major improvement over the 83 percent now covered, but the safety net would have holes.
Some 16 million eligible people would remain uninsured under the Senate bill and 12 million under the House bill, according to the Congressional Budget Office. That's not counting illegal immigrants, who would not be eligible for government assistance under either bill.
Both bills would eventually require Americans to get health insurance, or face fines.
Q: Why don't lawmakers just provide coverage for everyone?
A: Part of the reason is it would cost more, at least $250 billion over 10 years. The president wants to keep the total cost to about $900 billion. But it means workers and their families would be more than twice as likely to be uninsured as older people, virtually all of whom are now covered by Medicare.
Q: How affordable is the new middle-class coverage going to be?
A: It depends.
Most people would remain in their employer plans. Self-employed people and those working in small businesses would be able to buy coverage through a new insurance marketplace, with government subsidies available for many.
The aid is substantial for lower-income households, but drops off rapidly for the middle class.
Under the House bill, a family of four headed by a 45-year-old making $44,000 a year would pay roughly $2,400 in premiums, or $200 a month, according to the Kaiser Family Foundation.
A similar family making $66,000 would pay about $6,580 in premiums, or about $550 a month.
That's a bargain compared to current rates, which can top $1,000 a month, but it still may be too much for some family budgets. About one-third of the uninsured say they'd be able to pay $200 a month in premiums, and only 7 percent say they can afford $400.
Q: Twenty-year-olds don't have many health problems. Would they be required to get coverage?
A: You bet.
Unmarried children could stay on their parents' plan until age 27 in the House bill, 26 in the Senate plan. That change would start in 2010.
But those buying coverage for themselves could be in for sticker shock. Insurers now charge the young and healthy much less than middle-age people who are more likely to get sick. Under both bills, age-related premiums would be limited. So the young would pay more than they do now.
"The people who are going to do best are older people with a problematic medical history," said health policy expert Paul Ginsburg, of the Center for Studying Health System Change.
Q: These bills are going to ban pre-existing conditions, right?
A: Yes, but not immediately.
Both bills would forbid insurers from denying coverage to people in poor health or charging them more. That would happen in 2013 under the House bill, and 2014 in the Senate's.
The reason for the delay is that it would be unfair to require insurers to take all applicants right away. The sick would sign up, but healthy people would probably wait until they faced the threat of government fines. Such a situation could raise premiums for everyone.
Q: So if I have a health care problem, I might still have to wait three years to four years for coverage?
A: At Obama's request, lawmakers tried to take care of that by setting aside $5 billion for temporary "high-risk" insurance pools to provide affordable coverage for people whose health is frail.
But there's a problem with the patch.
According to the Congressional Budget Office, the money would run out in 2011 unless Congress pumps in more cash.
Q: Older people are concerned about what's going to happen to Medicare. Should they be?
A: Even though cuts in Medicare payments to hospitals and other providers are paying for much of the cost of covering the uninsured, benefits under traditional Medicare aren't reduced.
But those who've signed up for private insurance plans through Medicare Advantage could lose valuable extra benefits, according to the budget office.
For years, the government has been paying the private plans more than it costs traditional Medicare to deliver similar services. The plans used the money to provide extra benefits-mainly lower copayments and deductibles.
Both bills offer cheaper prescription drugs to those who fall into the "doughnut hole," the Medicare coverage gap. The House bill gradually would eliminate the gap. Both bills also provide better coverage for preventive care.
---------
"Plenty for retirees to like in health care reform measures"
By CHARLES BALBAN, Guest Commentary, nashuatelegraph.com/opinion/perspectives - Sunday, December 6, 2009
Remember the death panel scare? Health reform would allow the government to choose when you were going to die?
What a crackpot idea! It wasn’t true, but it sure raised a dust storm. The truth is, health reform has a lot to offer retirees.
What’s good: Health reform will make it easier for early retirees (55-64 years) to find and keep health insurance. The majority of these folks do not work full time. Many have pre-existing health conditions such as diabetes and heart disease. It’s hard for them to find and afford insurance. Health reform will help.
U.S. Reps. Paul Hodes and Carol Shea-Porter both voted for the House bill, America’s Affordable Health Choices Act. It would require insurance companies to cover individuals regardless of health status. It establishes exchanges that would allow early retirees to compare the bill’s public plan to private plans. It also would provide tax credits to people who earn up to 400 percent of the federal poverty level ($58,280 for two-person household). For someone earning about $22,000, the House bill would limit deductibles to $500.
What’s not so good: The Senate is debating a less realistic bill. It sets the deductible for that same $22,000 earner at $2,500.
What’s good: The House bill would lower out-of-pocket expenses for Medicare beneficiaries. We would never again have co-pays and deductibles for recommended preventive procedures such as colonoscopies, bone scans and diabetes screenings. It also would limit the amount private insurance companies can charge older people compared to 25-year-olds.
What’s good: Prescription drugs would be more affordable for Medicare enrollees. Currently, Medicare is not allowed to negotiate discount prices for drugs, thanks to pharmaceutical company lobbyists. Under the House bill, Medicare could negotiate discount prices and save billions.
The House bill uses these savings to close Medicare Part D’s cruel prescription drug coverage gap. It’s known as the “doughnut hole” for its now-you’re-covered, now-you’re-not structure.
Moderate-income Medicare enrollees whose prescriptions cost more than $2,700 per year often run up a credit card balance to buy prescriptions. Then they can’t pay off the balance because they drop into the doughnut hole again the following year. The House bill would close the gap over five years.
What’s not so good: The Senate bill does not close the gap. It does provide a 50 percent discount on brand-name prescription drugs for retirees who fall into the doughnut hole.
What’s good: When you hear that reform will “cut Medicare,” we’re talking about cutting fraud and drug company profits, and cracking down on wasteful subsidies to private insurance companies that offer Medicare Advantage plans.
The private MA plans were set up to compete with government-run Medicare and drive costs down. But they’ve failed. The financial tide ran the other way as Medicare poured $33 billion into these private companies between 2004 and 2008. This subsidy increased corporate profits but shortened the life of the Medicare Trust Fund by 18 months, according to the Commonwealth Fund.
Could cutting out the subsidy cost New Hampshire’s nearly 12,000 Medicare Advantage plan enrollees some extra benefits? It’s possible, if insurance companies choose to protect corporate profits instead of MA enrollees. (The House and the Senate bills both pull the plug on MA subsidies.)
What’s good: The House and Senate bills are funded by eliminating the Medicare Advantage subsidies, cutting fraud and taxing drug company profits. The House bill also would place a 5.4 percent surtax on taxes paid by individuals who earn more than $500,000 and a 2.5 percent excise tax on medical devices.
The Senate bill would charge fees to insurance and medical device manufacturers. It also would raise Medicare taxes slightly on individuals making more than $250,000 and places a 5 percent tax on elective cosmetic procedures.
What’s not so good: The Senate bill would tax health benefits provided to middle-class workers by their employers. That’s got to go.
This month you will hear the Senate debate a bill that does less for retirees than the House version. As you listen, give thanks to Reps. Paul Hodes and Carol Shea-Porter. They gave us the bill we need.
-
Charles Balban is president of the New Hampshire Alliance for Retired Americans.
-
---------
-

-
"Worries grow that health overhaul could price out many: Lawmakers weigh new subsidies to ease burden on struggling families"
By Lisa Wangsness, Boston Globe Staff, December 6, 2009
WASHINGTON - President Obama has promised that the nation’s health care overhaul will make medical insurance available - and affordable - for everyone. But while bills in Congress would make insurance more accessible for millions of Americans, advocates worry that the Senate bill would impose significant financial burdens on some of the families who will now be required to buy coverage.
It is a difficult and politically volatile problem for Democrats working toward passage of a sweeping insurance requirement heading into what promises to be a tough election year.
Bowing to consumer groups’ concerns about affordability, Democratic leaders have already added billions of dollars in subsidies to the proposal being debated on the Senate floor. But advocates remain concerned that even with that government help, premiums under the Senate measure would consume large portions of monthly budgets for families with low incomes.
“I think there’s still a significant problem for anyone who’s at the bottom end of the income scale in the Senate version,’’ said Michael Miller policy director of Community Catalyst, a Boston-based consumer health care advocacy group at the forefront of the affordability discussion.
Ron Pollack, executive director of Families USA, said that if the bill passes the Senate, advocates will try to persuade House and Senate leaders to adopt the contribution levels the House proposed for those with incomes at the lower end of the scale.
“For that group almost any out-of-pocket cost can be unaffordable,’’ he said.
Under the Senate proposal, most Americans would be required to buy health insurance. More than half of the people who could not get affordable coverage through their employers would be eligible for federally subsidized insurance, which could be purchased through an “exchange’’ - a new insurance market similar to the Massachusetts Health Insurance Connector. Those subsidies would cover nearly two-thirds of their insurance premium, according to congressional budget analysts - a huge savings for millions of families.
But advocates worry that such plans could still be too costly for some. A single mother of two with income of around $28,000 a year, for example, could have to pay more than $100 a month for insurance. In Massachusetts, the only state with a similar subsidized insurance system for people with low incomes, she would pay only $39.
“Those folks are just barely hanging on,’’ said Brian Rosman of Health Care for All-Massachusetts. “A lot of them are using credit cards to get by month to month.’’
Costs are also significant for middle-income families, a key demographic that Democrats want to cover, though the latest Senate bill is much more generous to them than previous versions.
Under the current Senate bill, a single mother of two earning $46,000 a year who could not get affordable insurance through work would have to pay about $300 a month for coverage. In the event of serious illness, she could have to pay up to $3,000 a year in out-of-pocket costs. A family of three earning just over $73,200 a year would have to pay $500 a month and up to about $4,000 a year out of pocket.
The House measure is more generous at the lower end of the income scale, but it would require higher premiums for middle-income people.
Those details could present political problems for lawmakers, specialists say.
“It’s the middle-income backlash that they actually have to worry about,’’ said Robert Blendon, a professor of health policy and political analysis at Harvard University. “It’s the $40,000 to $70,000 [income range] which has a lot of people in it who might think these sums are hard to pay.’’
Worried about just such a backlash, senators are offering an escape hatch: People would not be penalized for being uninsured if they could not find premiums that cost less than 8 percent of their incomes.
The government has estimated that by 2019, the Senate bill would reduce the number of uninsured people by 31 million, leaving 24 million non-elderly Americans without insurance. About one-third of the uninsured would be illegal immigrants, who would be barred from buying insurance through the new exchange.
For people earning three times the poverty level or less -about $55,000 for a family of three - premiums being contemplated in Washington are significantly higher than the ones offered in the pioneering Massachusetts health insurance program. The Bay State’s plan remains quite popular three years after its inception, in large part because subsidies are large and beneficiaries’ payments are low.
But the federal bills would be more generous than the Massachusetts law in one respect: In Massachusetts, those earning more than 300 percent above the poverty level are not eligible for subsidies; the federal measures would provide help for those at 400 percent of that level, or $66,000 for a family of three.
Some influential lawmakers say people should be able to buy lower-cost insurance plans with fewer benefits. The Senate bill would allow such plans to be offered through the exchanges, but only to people under 30 or to those who couldn’t find a plan that costs less than 8 percent of their income. Senators Susan Collins and Olympia Snowe, moderate Republicans from Maine whose votes are being courted by majority Democrats, say they may favor this approach.
“We are requiring people to spend a substantial amount of their income for insurance that in many cases is more expensive and has richer benefits than what most people are buying today in the individual market,’’ Collins said.
Democrats are also likely to continue discussing how to make subsidy levels more affordable
“It’s better than it was, and it has to get better,’’ said Senator Jay Rockefeller, Democrat of West Virginia, said just after the bill was brought to the floor.
But because President Obama has put a $900 billion limit on the bill’s overall price tag, and because the country is facing mounting deficits, Congress cannot offer unlimited subsidies to those who need help.
In 2006, when Massachusetts policy makers set out to determine how much people could afford to pay, the Greater Boston Interfaith Organization convened people in churches around the city and had them fill out monthly budgets detailing exactly how much they had left to spend on insurance after food, rent, utilities, bus passes, and other expenses.
Advocates analyzed the findings and brought them to the Massachusetts Health Insurance Connector Authority board, which factored that information in when it set standards for affordability, Rosman said.
“I think the way Congress needs to figure this out is to first see what people can afford and then devise a subsidy schedule that meets affordability,’’ he said. “They can’t put a price tag on the bill to start out with and try to fit [a] subsidy schedule into that price tag. You have to work the other way around, we would say.’’
In Massachusetts, a single mother of two earning $46,000 who cannot buy insurance through work only has to pay only about $116 a month for the least expensive plan available under Commonwealth Care, the state’s subsidized insurance program - about one-third of what the Senate and House proposals would require. The insurance Massachusetts offers through Commonwealth Care is generally comprehensive, so families who qualify pay very low out-of-pocket costs.
But Massachusetts also has several advantages that made it easier to offer more generous subsidies. A federal Medicaid waiver provided an extra injection of dollars, and higher rates of employer-based insurance meant that fewer people need help buying coverage.
A pool of money that had been used for care for safety net hospitals helps pay for the subsidies, and high-quality community-based managed care organizations such as the Cambridge Health Alliance have substantial experience providing care for low-income groups. The state has also chipped in hundreds of millions of dollars to help sustain the system.
It is unclear whether the Massachusetts subsidies would change if Congress approves a health care bill, but state officials are trying to make sure the state would not lower its standards.
-
www.boston.com/news/health/articles/2009/12/06/worries_grow_that_health_overhaul_could_price_out_many/?comments=all
-
---------
"Profit motive sickens health care"
The Berkshire Eagle, Letters to the Editor, December 16, 2009
Health care is a sick business. Imagine an entity that is both amoral and soulless, its guiding precept profit and growth. This is the foundation of the modern American conglomerate, including those of the health care, pharmaceutical and insurance industries.
According to the Huffington Post, health insurance giant Aetna is planning to force up to 650,000 clients to drop their coverage next year as it seeks to raise additional revenue to meet profit expectations. Information from an earnings conference call that was posted on the Web site seekingalpha.com indicates that in an effort to improve on a less-than-anticipated profit margin in 2009, Aetna would be raising prices on their consumers in 2010. Aetna actually made a profit in 2009 but not at levels that it anticipated, according to the Huffington Post. This is consistent with other insurers as well.
In May 2008, Wellpoint, one of the nation's largest private pay health plans, reported less-than-expected profits from the first three months of the year. According to amednews.com, they are cutting their rolls, increasing premiums and lowering physician re-imbursement to enhance profit margins. Could it be any more obvious that the only insurance business they are in is ensuring profit? Cutting their rolls and raising premiums will increase the numbers of uninsured, typically the sick, the elderly, and the poor, who in turn, will be added to government-run Medicare and Medicaid programs. If that isn't socialized medicine, what is?
The New York Times reported that even as drug makers promise to support Washington's health care overhaul by shaving $8 billion a year off the nation's drug costs after the legislation takes effect, in the last year, the industry has raised the wholesale prices of brand-name prescription drugs by about 9 percent, according to industry analysts. That will add more than $10 billion to the nation's drug bill, which is on track to exceed $300 billion this year.
Wow, what a concession: raising prices by more than $10 billion, conceding $8 billion, on their way to $300 billion annually, and growing! David Brennan, head of pharma giant AstraZeneca, when asked if he would oppose reform said: "We said there were principles we didn't want to see violated," according to the Huffington Post. "If those principles, price controls, Medicare rebates, moving dual eligibles back from Medicare and back into the Medicaid discount program happen, I can't see how we could be supportive of the program." In short, if health care reform does not guarantee increasing profit margins and growth, Big Pharma will oppose it.
It is precisely this profit-oriented approach to health care that has created and drives both, the disease crisis and its subsequent disease-care financial crisis in America. Does anyone really still believe we don't need reform? If so, what have you got to offer that can save us?
PETER D. MAY
North Adams, Massachusetts
-
www.topix.net/forum/source/berkshire-eagle/TPJJNSNP2JFBBS6BO
-
---------
"Who wins, who loses in Senate health bill"
By Erica Werner, Associated Press Writer, December 20, 2009
WASHINGTON --The little town of Libby, Mont., isn't mentioned by name in the Senate's mammoth health care bill, but its 2,900 citizens are big winners in the legislation, thanks to the influence of Finance Committee Chairman Max Baucus, D-Mont.
After pushing for years for help for residents, many of whom suffer from asbestos-related illnesses from a now-closed mineral mining operation, Baucus inserted language in a package of last-minute amendments that grants them access to Medicare benefits.
He didn't advertise the change, and it takes a close read of the bill to find it. It's just one example of how the sweeping legislation designed to remake the U.S. health care system and extend coverage to 30 million uninsured Americans also helps and hurts more narrow interests, often thanks to one lawmaker with influence or bargaining power.
Here's a look at some other winners and losers in the latest version of the legislation, which was expected to survive an initial test vote in the Senate around 1 a.m. Monday.
WINNERS
--Cosmetic surgeons, who fended off a 5 percent tax on their procedures.
--Nebraska, Louisiana, Vermont and Massachusetts. These states are getting more federal help with Medicaid than other states. In the case of Nebraska -- represented by Sen. Ben Nelson, who's providing the critical 60th vote for the legislation to pass -- the federal government is picking up 100 percent of the tab of a planned expansion of the program, in perpetuity. Vermont and Massachusetts get temporary increases in the federal share of their Medicaid tabs. In Louisiana, moderate Democratic Sen. Mary Landrieu negotiated $100 million for 2011 before announcing her support for the legislation.
--Beneficiaries of Medicare Advantage plans -- the private managed-care plans within Medicare -- in Florida. Hundreds of thousands of them will have their benefits grandfathered in thanks to a provision tailored by Sen. Bill Nelson, D-Fla., that also affects a much smaller number of seniors in a few other states.
--Longshoremen. They were added to the list of workers in high-risk professions who are shielded from the full impact of a proposed new tax on high-value insurance plans. (Electrical linemen were already included, along with policemen, firefighters, emergency first responders and workers in construction, mining, forestry, fishing and certain agriculture jobs.)
--Community health centers. They got $10 billion more in the revised bill, thanks to advocacy by Sen. Bernie Sanders, I-Vt.
--A handful of physician-owned hospitals being built around the country -- including one in Bellevue, Neb. -- which would be permitted to get referrals from the doctors who own them, avoiding a new ban in the Senate bill that will apply to hospitals built in the future. Without mentioning Nebraska or other states by name, the Senate bill pushes back some legal deadlines by several months, in effect making a few hospitals that are near completion eligible to continue receiving referrals from the doctors who own them. The provision was described by a pair of health industry lobbyists who spoke on condition of anonymity in order to speak freely. Chalk up another win for Nelson.
--AARP, the lobby for elderly people. The new Democratic bill has about $1 billion in extra Medicaid payments to states that provide visiting nurses and other in-home or community services to prevent low-income people from needing to be admitted to hospitals. In House-Senate bargaining, AARP also is expected to win one of their top priorities: a full closing of the so-called "doughnut hole," the gap in Medicare's coverage of prescription drugs.
--Doctors and hospitals in Montana, North Dakota, South Dakota, Utah and Wyoming, who will get paid more than providers elsewhere under formulas in the bill.
LOSERS
--Tanning salons, which are getting hit with a 10 percent tax on indoor tanning services, replacing the cosmetic surgery tax.
--Progressives. They had to give up on their long-held dream of a new government-run insurance plan so that Democratic leaders could lock down the necessary votes from moderates.
--People making over $200,000 a year. A proposed 0.5 percent increase in the Medicare payroll tax was bumped up to 0.9 percent in the latest version, putting the tax at 2.35 percent on income over $200,000 a year for individuals, $250,000 for couples.
--Generic drug makers. They fought unsuccessfully to block 12 years of protection that makers of brand-name biotech drugs -- expensive pharmaceuticals made from living cells -- will get against generic would-be competitors.
-
Associated Press writer Alan Fram contributed to this report.
-
---------
JEFF JACOBY: "Medicare and the Mayo Clinic"
By Jeff Jacoby, Boston Globe Columnist, January 6, 2010
PRESIDENT OBAMA is a great admirer of the Mayo Clinic. Time and again he has extolled it as an outstanding model of health care excellence and efficiency.
“Look at what the Mayo Clinic is able to do,’’ the president proclaimed at a rally in September. “It’s got the best quality and the lowest cost of just about any system in the country. . . . We want to help the whole country learn from what Mayo is doing.’’ On the White House website, you can find more than a dozen examples of Obama’s esteem.
So perhaps the president will give some thought to the clinic’s recent decision to stop accepting Medicare payments at its primary care facility in Glendale, Ariz. More than 3,000 patients will have to start paying cash if they wish to continue being seen by doctors at the clinic; those unable or unwilling to do so must look for new physicians. For now, Mayo is limiting the change in policy to its Glendale facility. But it may be just a matter of time before it drops Medicare at its other facilities in Arizona, Florida, and Minnesota as well.
Why would an institution renowned for providing health care of “the best quality and the lowest cost’’ choose to sever its ties with the government’s flagship single-payer insurance program? Because the relationship is one it can’t afford. Last year, the Mayo Clinic lost $840 million on its Medicare patients. At the Glendale clinic, a Mayo spokesman told Bloomberg News, Medicare reimbursements covered only 50 percent of the cost of treating elderly primary-care patients. Not even the leanest, most efficient medical organization can keep doing business with a program that compels it to eat half its costs.
In breaking away from Medicare, the Mayo Clinic is hardly blazing a trail. Back in 2008, the independent Medicare Payment Advisory Commission reported that 29 percent of Medicare beneficiaries who were looking for a primary-care doctor were having difficulty finding one willing to treat them. A survey by the Texas Medical Association that year found that only 38 percent of the state’s primary-care physicians were accepting new Medicare patients.
But if you think that sounds grim, wait until Congress enacts the president’s health care overhaul. A central element of both the House and Senate versions of ObamaCare is that Medicare reimbursements to hospitals and doctors - already so low that many providers lose money each time they treat a Medicare patient - will be forced lower still.
The Centers for Medicare and Medicaid Services, a branch of the US Department of Health and Human Services, estimated last month that the Senate bill would squeeze $493 billion out of Medicare over the next 10 years. As a result, it cautioned, “providers for whom Medicare constitutes a substantive portion of their business could find it difficult to remain profitable and . . . might end their participation in the program (possibly jeopardizing access to care for beneficiaries).’’ In short, the Democratic understanding of health care reform - more government power to set prices, combined with reduced freedom for individuals - will make medical care harder to come by: an Economics 101 lesson in the pitfalls of price controls.
Nearly six months ago, the Mayo Clinic tried to sound an alarm. Instead of making American health care better and more affordable, it warned, the legislation working its way through Congress “will do the opposite’’ and “the real losers will be the citizens of the United States.’’
Each year Medicare loses tens of billions of dollars to fraud and abuse. The program’s long-term deficit is a staggering $38 trillion. Its expenditures have raced ahead of inflation from the day it was created: Medicare’s price tag has skyrocketed from $3 billion in 1966 to $453 billion this year. Yet its reimbursement of medical providers is so meager that more and more of them cannot afford to treat Medicare patients. Whatever else Medicare might be, it is no model for rational reform.
Obama says he wants the country to “learn from what Mayo is doing.’’ What Mayo is doing is trying to provide high-quality medical care in the face of Washington’s compulsively misguided interference. As 3,000 Mayo patients have just learned, government interference can hurt. Ratchet up that interference with ObamaCare, and the pain will grow worse.
-
Jeff Jacoby can be reached at jacoby@globe.com.
-
---------
"Expect higher health care costs in 2010"
By Pat Regnier, Money Magazine assistant managing editor, December 29, 2009
(Money Magazine) -- Last month was open-enrollment season, and my wife and I got an unpleasant surprise. For 2010 we're looking at an annual health-insurance premium that's $1,600 higher than it is now, plus higher deductibles. Instead of flat co-pays, we'll pay co-insurance, a share of the total costs. And this is with a plan provided by a Fortune 500 company that still spends big bucks on relatively generous benefits.
You may well be in the same boat. According to human-resources consultant Hewitt Associates, the average large-company employee will pay $4,023 in premiums and out-of-pocket costs next year -- 10% more than in 2009 and more than three times the level in 2001.
We are witnessing the slow death of what some political scientists dub the corporate welfare system. Until quite recently employees of giant companies essentially lived in Canada, but with shorter lines for the MRI machines. That is, they didn't have to think very hard or very often about medical expenses.
But the relentless increase in health-care costs is unraveling those arrangements year by year. And for many people at smaller firms -- not to mention the self-employed -- those days are already long gone.
You'll miss those co-pays
Hewitt's Cathy Tripp calls the shift from co-pays to co-insurance -- the big trend this year -- "cost transparency." You'll feel the true cost of doctor visits, the thinking goes, and therefore spend less.
But hospitals don't yet post their prices for procedures the way Target does for dish soap. The delivery of my second child wound up costing $1,000 more than that of our first just two years earlier. I have no idea whom I would have talked with to figure out that tab ahead of time.
For families, the new "transparency" can actually feel pretty murky. It makes it harder for them to predict what their medical costs will be in a given year.
It won't get simple soon
There are two schools of thought on why health care is so expensive. And there's truth in both. The first says that patients are ignorant of costs. (The prescription: more of those out-of-pocket payments.) The second looks at the pricing power of doctors and hospitals, as well as their financial incentives.
Years of research out of Dartmouth have documented that spending on health can vary wildly from one region to another, but that the places spending more don't get better health results. Ideally, you want providers to focus on getting you well with just as much treatment as will help and not a scan or pill more. But our piecework system of paying for care rewards them for doing more things.
The health bills now before Congress have some measures that try to change how health providers are paid. But they'd just be a start. (Most have to do with how Medicare pays its bills, not what your insurer does.)
The fact is, cost control will be a year-by-year exercise in political will, not a single bill. We've had some practice cranking the "more out-of-pocket" lever to address rising health costs. The "pick a fight with docs and hospitals" lever may be harder for Washington to pull.
---------
"Health insurance rates soar for some"
By Linda A. Johnson, Associated Press, February 13, 2010
TRENTON, N.J. -- Consumers in at least three states who buy their own health insurance are getting hit with premium increases of 15 percent or more.
Anthem Blue Cross, a subsidiary of WellPoint Inc., has been under fire for a week from regulators and politicians for notifying some of its 800,000 individual policyholders in California that it plans to raise rates by up to 39 percent March 1.
The Anthem Blue Cross plan in Maine is asking for increases of about 24 percent this year. Last year, they raised rates 32 percent.
And in Oregon, multiple insurers were granted rate hikes of 15 percent or more this year after increases of around 25 percent last year.
The increases affect groups of customers who purchase individual health insurance, rather than getting it through their employer.
Premiums are far more volatile for individual policies than for those bought by employers and other large groups, which have bargaining clout and a sizable pool of people among which to spread risk. As more people have lost jobs, many who are relatively healthy have decided to go without health insurance or get a bare-bones, high-deductible policy. Both result in a decline in premiums for insurers.
Steep rate hikes in this sliver of the insurance market have popped up sporadically for years. Experts see them becoming increasingly common.
"You're going to see rate increases of 20, 25, 30 percent" for individual health policies in the near term, Sandy Praeger, chairwoman of the health insurance and managed care committee for the National Association of Insurance Commissioners, predicted Friday.
A number of consumer groups in Maine are planning big rallies at two public hearings on Anthem's proposed rates later this month.
Politicians and even some health insurers are urging a revival of the stalled effort in Congress to overhaul the health care system.
WellPoint, which is based in Indianapolis, has said it needs to raise rates so much because the weak economy has resulted in a smaller number of people, many with serious health problems, remaining in the individual market in the individual market in California, while costs of caring for them have been rising due to higher provider prices and more use of diagnostic tests.
About 13 million Americans purchased health insurance through the individual market in 2008, the most recent data available.
-
www.topix.net/forum/source/berkshire-eagle/TI6SGL8BCDRURUOB4
-
---------
"No shame among insurers"
The Berkshire Eagle, Editorials, February 15, 2010
The nation's five largest health insurance companies increased their profits by 56 percent in 2009 while covering 2.7 million fewer people than in 2008. In some cases, money spent on medical care was cut while salaries went up and profits increased. This is the system minority Republicans in Washington are determined to preserve, even though it is financially crippling American workers and their struggling employers.
The now-dead public option would have given Americans an alternative to profit-first insurers and would have provided a powerful incentive for insurance companies to behave responsibly. Instead we have the disgraceful spectacle of Anthem Blue Cross, a California subsidiary of WellPoint, one of the five insurers whose public records were analyzed by Health Care for America Now, raising premiums this year by as much as 39 percent on some individual policies.
With the conservative judicial activists on the Supreme Court having sold out the American electoral process to corporations like the five sited by Health Care for America Now - WellPoint, UnitedHealth Group, Cigna, Aetna and Humana - it isn't difficult to predict which legislators will be rewarded. Follow the health insurer money in 2010 and 2012.
-
www.topix.net/forum/source/berkshire-eagle/TTIQLHPMKQBC3M9EK
-
---------
"Consequences of health reform failure"
By Charles Joffe-Halpern, The Berkshire Eagle, Op-Ed, February 17, 2010
NORTH ADAMS, Massachusetts
In this emotional and polarized political environment, while the procedural challenges to successfully pass comprehensive national health reform have become more formidable, we should not forget that the consequences are too high to let health reform fail.
It is anticipated that without health reform, by 2019 the number of uninsured in the United States will reach between 54 million to 67 million, most of them middle-income adults. Health care costs will continue to rise, businesses could see their health care costs double within 10 years, and the trend of employers dropping health coverage will continue to spiral. Not to be overlooked, health insurers will be able to continue denying coverage to people with pre-existing conditions.
It is important to keep in mind that both the U.S. Senate and the House of Representatives have now passed similar comprehensive health reform bills that address this inevitability. Before the special Massachusetts election, while there were differences that needed to be reconciled, the House and Senate were days away from finalizing the compromises needed to pass the final legislation.
*
The key features of both bills include:
-- Providing subsidies to help pay for health insurance for individuals with incomes up to under $43,320 a year who are not offered health coverage through their employer. These are higher eligibility guidelines than the current subsidized Massachusetts plan, and will enable an additional 75,000 Massachusetts to afford health coverage.
-- Implementing a nationwide health insurance mandate similar to the Massachusetts model.
-- Regulating insurers so they would no longer be able to exclude applicants based on pre-existing conditions, or charge higher premiums for those with pre-existing conditions.
-- Providing subsidies to small businesses to help them purchase coverage.
-- Improving the Medicare drug program by closing the costly gap in coverage referred to as the donut hole.
-- Working toward cost control by adopting payment mechanisms that would put pressure on costs by rewarding more efficiently provided, coordinated care and working toward making Medicare a more cost effective program.
It is projected that at least 30 million currently uninsured individuals will be covered under the health reform bill.
For Massachusetts, it is also important to understand that national health reform will provide increased federal funding, up to $750 million over five years, to supplement our current state health care costs.
Later this month, President Obama will be meeting with Republican leaders in an attempt to explore bi-partisan consensus on how to pass health reform. There is little optimism this meeting will result in an agreement on how to move forward. If, as expected, the outcome of this meeting is unsuccessful, the path to passage will be for the House to pass the current Senate bill with a set of amendments making the bill more acceptable to both chambers. These amendments can be passed through the budget reconciliation process.
Despite protests to the contrary, there is nothing controversial or extraordinary about this process. President George W. Bush used budget reconciliation five times to move his legislative agenda forward, including his three major tax cuts, and in 1994 Congress used reconciliation to enact President Bill Clinton's budget.
*
Before the special Massachusetts election, for the first time in our history, the country was on the verge of passing health care legislation that embraced the principle that all Americans deserve to have access to affordable health coverage. Many progressive Democrats are disappointed the bill doesn't go far enough toward guaranteeing coverage for all, and with partisan lines drawn, Republicans feel the government will be playing too big a role in our health care system.
The reality is the current health reform bill is already a compromise. We cannot let fatigue with the legislative process, or fear of changing the status quo keep us from moving forward; it is the maintaining status quo that should be feared. The consequences of inaction will be intolerable.
-
Charles Joffe-Halpern is the executive director of Ecu-Health Care in North Adams and the president of Health Care for All in Boston.
-
www.topix.net/forum/source/berkshire-eagle/TTKQS74IEVM8KP6VL
-
---------
"Medicaid enrollment rises nationwide, analysis finds"
By Amy Goldstein, Washington Post Staff Writer; A04, February 19, 2010
The recession has fueled the greatest influx of Americans onto Medicaid since the earliest days of the public insurance program for the poor, according to new findings that show caseloads have surged in every state.
More than 3 million people joined Medicaid in the year that ended in June, the data released Thursday show. That pushed enrollment to a record 46.8 million, exacerbating the financial strains on already burdened states and complicating the federal politics of health care.
The analysis by the Kaiser Family Foundation, a health policy and research organization, found that in three-fifths of the jurisdictions, including Maryland and the District, people rushed into the safety net for health coverage at more than twice the rate as the year before.
Medicaid directors said in interviews that despite early clues elsewhere that the economy may be starting to improve, the demand for government health coverage has not tapered off since last summer. "Nope. It hasn't slowed down yet," said John Folkemer, deputy secretary for health-care financing for Maryland, where the caseload rose by 20 percent from June 2008 to June 2009, the steepest increase in the country.
Like the rising demand for food stamps and welfare benefits, the increase in people turning to Medicaid reflects the millions of Americans who have lost jobs and economic self-reliance and are asking the government for basic help, in many instances for the first time.
Because the program is large and expensive, the spurt in Medicaid caseloads has produced far more damaging effects on state budgets than the other two programs. In the past year or two, many states have responded by reducing the medical services available to Medicaid patients or payments to doctors, hospitals and other providers of health care.
Now, 29 states are considering further reductions or have made them since their current fiscal year began, Thursday's report said. Such strains exist even though the federal government has been giving states extra money for Medicaid as part of the economic stimulus efforts Congress set in motion a year ago. The extra subsidies are due to expire at the end of this year, and states are lobbying hard to continue them for at least six months.
The worsening financial burden imposed by Medicaid also has heightened some governors' wariness about the approach to redesigning the nation's health-care system that is favored by the White House and congressional Democrats. In the health-care bills passed by the House and the Senate, an expansion of health coverage to the uninsured would rely substantially on Medicaid. If the legislation were enacted, the federal government would pick up the cost for the first few years, but, after that, states would contribute a small portion.
"Reform is needed, but, gosh, the hard nut to crack is, how do you fund it?" said Charles Duarte, the administrator who oversees Medicaid in Nevada, where the caseload rose 13 percent in the year that ended in June.
Medicaid, created as part of the Great Society policies of the mid-1960s, is a shared responsibility of the federal government and states. The federal government pays part of the cost, depending on each state's wealth, and requires a certain level of coverage, but states are free to set many of their program's rules, including whether to furnish additional benefits.
In the Washington area, which has many low-income residents who have long relied on government help, the Medicaid rolls rose by 4 percent, compared with a 1 percent increase a year earlier. Virginia's caseload increased by 8 percent, compared with slightly more than 4 percent the previous year.
In Maryland, Folkemer, the Medicaid director, said that perhaps two-fifths of more than 100,000 extra people in the program signed up because of a change in summer 2008 that allowed more parents to enroll. But most of the increase, he said, "was because of the economy."
Maryland is one of a few states in which, even during the economic downturn, policymakers have tried to broaden access to public insurance. Wisconsin Gov. Jim Doyle (D) said that in the past four years, the state has taken steps to expand BadgerCare, as the state calls both Medicaid and its version of the State Children's Health Insurance Program. "We have continued on, even in the face of the economic crisis," Doyle said in an interview, so that Wisconsin now has the nation's second-lowest portion of uninsured residents, after Massachusetts.
In most states, however, the growth of Medicaid is a result of economic bad times. By the end of 2009, Nevada's Medicaid rolls had shot up 20,000 above the 220,000 the state had forecast, Duarte said. Next week, he said, the state's legislature, faced with revenue far lower than expected from gambling and sales, will hold special sessions to cut the budget.
Last summer, Duarte said, he was able to restore several reductions in benefits the legislature had cut not long before, including vision coverage and some dental care for adult Medicaid patients. Now, he said, as legislators look for new cuts, that list of services "is back on the table, with more added to it."
-
Correction to This Article
This article about increases in Medicaid caseloads across the country incorrectly said that, in the Washington area, Medicaid rolls rose by 4 percent during the year that ended in June, compared with a 1 percent increase the year before. Those figures are for the District, not the region. There were no figures available for the Washington area as a whole.
-
---------
-
My Daily Work: "Health coverage"
-

-
Posted by Dan Wasserman, The Boston Globe, February 24, 2010
-
---------
-

-
2/19/2010
-
---------
"Health-care legislation's insurance subsidies prompt questions of affordability"
By Amy Goldstein, Washington Post Staff Writer, A04; March 20, 2010
The final health-care legislation that House Democrats are striving to pass this weekend would give about 19 million Americans subsidies averaging $6,000 to help pay premiums and other insurance charges, an unprecedented government investment in private health policies that leaves lingering questions about whether coverage would truly become affordable.
The details of the subsidies, which emerged in the past day, provide the clearest picture yet on a central question that has hovered over the health-care debate since it began a year ago: How much help would the government give people to cope with the expense of medical insurance?
In the final version Democrats produced, the subsidies would be part of a two-prong approach by the government to extend coverage to the vast majority of people who are uninsured. That effort is predicted to cost nearly $800 billion, more than $4 of every $5 of the legislation's total cost.
The private insurance subsidies would begin in 2014 and be intended for people eligible to buy coverage through insurance exchanges that would be created the same year.
The money the government spends to subsidize private policies would eclipse that devoted to a historic expansion of Medicaid, according to House aides and congressional budget analysts. And the subsidies are tilted more toward lower-income Americans than the measures in the Senate's version of health-care legislation.
The large infusion of federal money into insurance coverage would address one of the twin goals that have been at the heart of every attempt to redesign the nation's health-care system for decades: making health care more accessible and slowing medical costs. As Congress approaches what Democrats on Capitol Hill and in the White House are heralding as the finale of a year-long debate, policy experts across the ideological spectrum differ over how well the legislation would succeed at either goal.
Even some proponents of the subsidies say that, generous as they are, their buying power could erode over time in an era of rapid medical inflation. Some critics say the Democrats' approach of creating state insurance exchanges would help some Americans, those who now look for insurance policies individually or in small groups, but provide fewer new purchasing alternatives to most Americans, who rely on coverage through their jobs.
Still, liberal groups eager for the health-care legislation to pass are heaping praise on the final version of the subsidies, released Thursday among a set of changes to the Senate bill. "This is a huge step in the direction of making coverage and care affordable," said Ron Pollack, executive director of Families USA, a left-leaning consumer health lobby.
Specifically, the subsidies would come in two parts, both available on a sliding scale to Americans with incomes too high for Medicaid. That would span families of four with incomes from $29,000 to $88,000 and individuals with incomes from $14,000 to $43,000.
One part of the subsidies would consist of tax credits to help Americans afford insurance premiums, guaranteeing that they would not spend more than a specific portion of their income for them, ranging from 3 percent to 9.5 percent. Those subsidies, estimated to cost $40 billion over the next decade, would be less generous than envisioned by the House in the original health-care bill it adopted in the fall but more generous than the Senate version.
The second part of the subsidies, estimated to cost $466 billion during the next decade, would limit out-of-pocket expenses for deductibles and co-payments. This help, for individuals with salaries of $27,000 and families with income of $55,000, would be significantly more generous than any version of the legislation Congress has considered.
Although the financial help would be designed mainly for Americans who cannot get coverage through their employers, the legislation also would allow workers to buy policies through an insurance exchange -- and get the subsidies if they qualify -- if their employers compelled them to pay too much for premiums, more than 9.5 percent of their income.
Despite that feature, Douglas Holtz-Eakin, a Congressional Budget Office director under President George W. Bush, criticized the subsidies for what he called "the inequity thing." He said, "You are setting up a system where two people making the same [income] are treated very differently," depending on whether they work somewhere that offers insurance. He predicted that difference could eventually place pressure on Congress to subsidize more Americans.
Edward F. Howard, executive vice president of the Alliance for Health Reform, said the subsidies would help "as many people as you can for as long as you can." But he cautioned that, over time, if medical costs continue to rise at the rampant pace of recent years, the federal help would increasingly fall behind. The annual adjustment to the subsidies would start out slightly higher, but starting in 2019, would become tied to the inflation rate. "The screws will tighten," he said.
---------
-
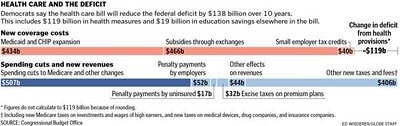
-
via The Boston Globe on March 21, 2010
-
---------
"THE INFLUENCE GAME: Drug lobby's health care win"
By Alan Fram, Associated Press Writer, March 29, 2010
WASHINGTON – Chalk one up for the pharmaceutical lobby. The U.S. drug industry fended off price curbs and other hefty restrictions in President Barack Obama's health care law even as it prepares for plenty of new business when an estimated 32 million uninsured Americans gain health coverage.
To be sure, the law also levies taxes and imposes other costs on pharmaceutical companies, leaving its final impact on the industry's bottom line uncertain. A recent analysis by Goldman Sachs, the Wall Street firm, suggests the overhaul could mean "a manageable hit" of tens of billions of dollars over the coming decade while bolstering the value of drug-company stocks. Others expect profits, not losses, of the same magnitude.
Either way, pharmaceutical lobbyists won new federal policies they coveted and set a trajectory for long-term industry growth. Privately, several of them say their biggest triumph was heading off Democrats led by Rep. Henry Waxman, D-Calif., who wanted even more money from their industry to finance the health care system's expansion.
"Pharma came out of this better than anyone else," said Ramsey Baghdadi, a Washington health policy analyst who projects a $30 billion, 10-year net gain for the industry. "I don't see how they could have done much better."
Costly brand-name biotech drugs won 12 years of protection against cheaper generic competitors, a boon for products that comprise 15 percent of pharmaceutical sales. The industry will have to provide 50 percent discounts beginning next year to Medicare beneficiaries in the "doughnut hole" gap in pharmaceutical coverage, but those price cuts plus gradually rising federal subsidies will mean more elderly people will purchase more drugs.
Lobbyists beat back proposals to allow importation of low-cost medicines and to have Medicare negotiate drug prices with companies. They also defeated efforts to require more industry rebates for the 9 million beneficiaries of both Medicare and Medicaid, and to bar brand-name drugmakers' payments to generic companies to delay the marketing of competitor products.
The impressive list of wins is testament to a carefully planned and well-financed lobbying strategy, led by Pharmaceutical Research and Manufacturers of America, the industry's deep-pocketed trade group.
The trade group has been led by Billy Tauzin, whose $4.5 million in earnings in 2008, the most recent figure available, underscore the high stakes for the industry.
The former Louisiana congressman will quit his post in June — a decision he abruptly announced in February when it seemed the health bill would die. Some industry officials said at the time that Tauzin was forced out, which the trade group denied.
As Obama's health care drive began last year, drugmakers agreed with Senate Finance Committee Chairman Max Baucus, D-Mont., and White House officials to support the effort. In exchange, the companies volunteered $80 billion in 10-year savings for the health care changes, and backed it up with an expensive TV ad campaign pushing Obama's proposal.
It is unclear precisely how much drug manufacturers ended up contributing, in part because much of the savings — like discounts to seniors — come off prices the companies themselves set. Their biggest expenses over the decade are estimated to include over $20 billion for an expanded rebate for medicines used by Medicaid, $28 billion for a new fee on drug firms and about $30 billion for closing the "doughnut hole."
In a March 21 newsletter, the financial services firm Morgan Stanley estimated a $95 billion, 10-year price tag, offset by tens of billions the companies would gain from extra customers and other provisions. Industry critics say the cost will be lower because of firms' control of prices, and will be more than outweighed by added sales.
Yet even the worst-case scenario — a net cost of tens of billions — would be small for a U.S. drug industry that IMS Health, a medical data firm, calculates earns more than $300 billion a year.
"Let's put it this way: They can afford it," said Tim Chiang, a pharmaceutical analyst in Stamford, Conn.
Drugmakers gained an eleventh-hour win when lawmakers decided against expanding drug discounts to some hospitals serving low-income patients, a proposal some feared could cost tens of billions. The overhaul law that Obama signed Tuesday would have broadened those discounts to inpatients, but the companion bill revising the earlier measure largely pulled that back.
Senate Finance Committee Chairman Baucus, said in an interview last week that as a trade-off for rolling back that expansion, the drug industry agreed to provide an additional $10 billion over a decade to help close the gap in Medicare coverage.
As for what Democrats gained from their ally, the industry and coalitions it joined spent about $67 million on supportive TV ads since the beginning of 2009, according to Evan Tracey, president of Kantar CMAG, which tracks political ads. That made it one of the biggest players in an airwaves battle that saw all sides spend $220 million.
Pharmaceutical interests spent $188 million lobbying last year, more than all but a handful of industry sectors, according to the nonpartisan Center for Responsive Politics. They employed an army of 1,105 lobbyists.
And after years of funneling most of its campaign contributions to Republicans, the industry has favored Democrats with 56 percent of the $5 million it has handed candidates so far this year. The biggest recipient, by far, of the industry's 2008 election cycle contributions of $13.8 million was Obama, who received $1.2 million for his presidential campaign.
"They're certainly going to get a very high return on that investment," Waxman said in a recent interview.
---------
-

-
Gov. Deval L. Patrick said he opposed rate increases because small businesses and working families needed financial relief. (Gretchen Ertl for The New York Times).
-
"Massachusetts Insurance Regulators Reject Most Requests for Higher Rates"
By KEVIN SACK, The New York Times, April 1, 2010
With the encouragement of Gov. Deval L. Patrick, Massachusetts insurance regulators took the extraordinary step Thursday of rejecting nearly 9 out of 10 rate increases requested by the state’s health insurers.
Mr. Patrick, a Democrat who is running for re-election, most likely against a former health insurance executive, said the move was needed because “small businesses and working families can’t wait any longer” for relief. The requested premium increases, which were for individual and small-group plans, ranged from 7 percent to 34 percent.
Small businesses cheered the state’s intervention, but health insurers predicted disruption in the marketplace, including voided contracts and legal challenges. They said Mr. Patrick’s main target seemed to be his leading Republican challenger, Charles D. Baker Jr., the former chief executive of Harvard Pilgrim Health Care.
Mr. Patrick’s move, which Mr. Baker dismissed as “an election-year gimmick,” reflects the political advantage that many candidates perceive in attacking health insurance rates this year. Some analysts considered it a turning point in the health care debate in Washington when the Obama administration highlighted double-digit increases announced by Anthem Blue Cross of California.
“Right now, premium increases have never been more political,” said Sandy Praeger, the insurance commissioner in Kansas and past president of the National Association of Insurance Commissioners. “If there is any way to justify not granting the increase, commissioners are looking for them.”
President Obama proposed in February that the federal government be given new powers to rule on whether premium increases are justified and to force insurers to reduce them.
In the end, Congress did not go that far. The new law requires that the administration review premium increases annually, beginning this year. When rates are considered unreasonable, insurers will have to justify them publicly. But the law does not allow the federal government to control prices, leaving that authority to the states.
States vary widely in regulation of insurance pricing. In California, for instance, the insurance commissioner, Steven Poizner, is reviewing Anthem’s proposed increases of up to 39 percent. But he can deny them only if he finds that the company is not spending at least 70 percent of premiums on health claims, as required by state regulations.
In Massachusetts, the power to disapprove rates has been vested in the insurance commissioner since 1977. That authority had never been used before Thursday, said Insurance Commissioner Joseph G. Murphy, who was appointed by Mr. Patrick.
In February, at Mr. Patrick’s direction, the state’s Insurance Division required health insurers to give the state 30 days’ notice to review proposed rate increases scheduled to take effect April 1. Previously, insurers simply filed their increases when the new rates started, and they were rubber-stamped by regulators.
But on Thursday, Mr. Murphy denied 235 of the 274 proposed increases. He said he disapproved requests when companies significantly exceeded the region’s medical inflation rate of 5.1 percent, failed to justify why varying rates were paid to different hospitals, and did not forcefully negotiate prices with providers.
Insurers have a right to appeal, and rates from the previous year stay in effect in the meantime. Consumers will receive refunds or credits if they have already started paying higher rates.
Mr. Murphy said his department estimated that the denials would save consumers — and thus cost insurers — $6 million to $8 million a month.
Lora M. Pellegrini, the president of the Massachusetts Association of Health Plans, called the denials “a very reckless act” and warned that insurers on thin margins might have trouble paying claims. Three of the state’s four largest health insurers reported operating losses last year.
Ms. Pellegrini said the timing of the announcement suggested that it was “largely political.” She said Mr. Patrick should focus attention on the primary cause of health care inflation, which she identified as rising medical costs.
A Boston University study recently found that hospital costs per Massachusetts resident were 55 percent higher than the national average. An investigation this year by the state attorney general concluded that the pricing leverage exerted by academic medical centers played a major role.
“Arbitrary government price controls will not solve the problem and will likely cause unintended harmful consequences,” the state’s largest insurer, Blue Cross Blue Shield of Massachusetts, said in a statement.
Ms. Pellegrini warned that government rate regulation would splinter the coalition of stakeholders who have supported the state’s pioneering universal coverage law.
“This feels like an unraveling of all that good work,” she said.
But Barbara B. Anthony, the state under secretary for consumer affairs, who oversees the Insurance Division, said the state had studied whether the rate denials would pose a threat to solvency.
“During times like this,” Ms. Anthony said, “it’s unfortunate, but reactions tend to be hyperbolic and exaggerated.”
Mr. Patrick has said the price controls are needed as a bridge until the legislature can act on his administration’s proposal to restructure the way doctors and hospitals are paid. The governor and Democratic lawmakers are working to construct a system that would pay health care providers collectively to keep patients healthy while eliminating incentives that encourage unneeded treatment.
Mr. Patrick has also proposed legislation that would give the state new authority to reject unreasonable hospital and physician prices, just as it did Thursday with insurance premiums.
---------
"Health insurance group to sue state over premiums"
By Christine McConville, Healthcare, bostonherald.com - April 5, 2010
The state’s six health insurers filed suit today against Massachusetts Division of Insurance Commissioner Joseph G. Murphy, saying he acted illegally when he told insurers to charge their customers last year’s lower rates.
“He had no authority to establish rates,” said the insurers’ lawyer, Dean Richlin, a partner at Foley Hoag.
Insurance division spokesman Jason Lefferts said the state agency is working on a response to the lawsuit.
Attorneys for the two factions are expected to face off Thursday morning at Suffolk Superior Court when Richlin plans to ask the judge to temporarily allow his clients to charge customers the higher rates, which Murphy rejected. Richlin said his clients are prepared to go to trial as soon as June 15.
Last week, the insurance division denied 235 of 274 rates proposed by health insurers.
Murphy said the rejected rates were “unreasonable relative to the benefits provided.”
It was the first time the state has used emergency authority to reject health insurance premium increases.
Today, the Massachusets Association of Health Plans, which represents four of the five state health insurers, teamed up with Blue Cross Blue Shield of Massachusetts to fire back.
In a statement, MAHP said “the rates that the health plans filed for April 2010 are actuarially sound, which is the basis upon which the Division’s decision should have been made.
“The Division’s decision has capped rates at levels it knows are insufficient to cover the cost of medical services and will result in collective losses to the state’s not-for-profit health plans that will exceed well over $100 million in 2010,” they added.
---------
"Health insurers shifting costs ahead of law: report"
By Susan Heavey, April 15, 2010
WASHINGTON (Reuters) – Some of the largest U.S. health insurers are changing their accounting practices to book administration costs as medical costs in an attempt to circumvent new industry reforms, according to a U.S. Senate panel's report released on Thursday.
Under the healthcare law passed in March, insurers must adjust their spending habits to meet new requirements. For example, large group plans must spend at least 85 cents of every premium dollar paid to them on actual medical care as opposed to administrative costs, while individual and small group plans must spend 80 cents.
Wall Street closely watches such spending levels, known as medical-loss ratios, or MLRs, as a sign of potential profits. Major health insurance stock indexes fell after the report.
"The insurance industry is beginning to consider the financial impact of the new federally required (medical) loss ratio requirements, including questionable changes in their accounting practices," the Democratic-led Senate Committee on Commerce, Science and Transportation said in a statement.
For example, WellPoint Inc "has already 'reclassified' more than half a billion dollars of administrative expenses as medical expenses," it said.
WellPoint spokeswoman Kristin Binns said the company would work with regulators to implement the MLR requirement, but did not comment on whether it had shifted any costs or changed its accounting practices.
A review of companies' expenses for 2009 shows that in some markets, insurers are spending 74 cents per dollar on care on average, according to the report, which was released on the committee's website at http://link.reuters.com/bas87j.
Cigna spokesman Chris Curran said it was too early to say how the new MLR rules would affect the insurer, and that methods of calculating costs were still being developed ahead of the new rules. Other insurers did not respond to requests for comment.
2011 DEADLINE
Although the MLR rule does not kick in until January 1, insurers so far are "still far below" what the law will require, said Senator John Rockefeller, the committee's chairman.
"This new data makes clear that too many health insurance companies are still putting profits before people," Rockefeller said, "and they have a lot of work to do to meet the consumer protection requirements of the health care reform law by the end of this year."
Regulators at the Department of Health and Human Services, charged with implementing much of the new health reform law, are pushing to apply the MLR changes quickly.
Earlier this week, the agency called on a major health insurance organization -- the National Association of Insurance Commissioners -- to give its recommendations for specific MLR ratio regulations by June 1, six months earlier than the law's December 31 deadline.
"(The agency) is seeking to publish regulations as soon as possible to allow sufficient time for health insurance issuers to incorporate these changes," U.S. Health Secretary Kathleen Sebelius wrote in a letter the group.
The S&P Managed Health Care Index closed down 0.9 percent on Thursday. The Morgan Stanley Healthcare Payor Index, which also fell after the report was released and was largely in negative territory all day, closed up 0.4 percent.
(Reporting by Susan Heavey; Editing by Lisa Von Ahn and Tim Dobbyn)
---------
"Health Bill Taps Into States' Medicaid Funds"
By Christopher Weaver, NPR, April 21, 2010
The new health care law could shift billions of dollars from cash-strapped states to the federal government by changing the way Medicaid prescription drug rebates are treated, according to state and industry officials and an examination of Medicaid spending data.
Democrats included a provision in the health law designed to raise $38 billion over 10 years by requiring greater discounts from drugmakers selling to Medicaid, the joint federal-state health insurance program for the poor. Previously, the rebates were divided between the states and the federal government. Under the law, a significant portion of the rebates will go solely to Washington beginning this year.
Regan Lachapelle, a spokeswoman for Senate Majority Leader Harry Reid, D-Nev., said the change was necessary to help pay for a $434 billion, 10-year increase in federal Medicaid funding. "Federalizing the rebate was a small piece compared to the many things we did to help states," she said in an e-mail.
In addition, for some states, the rebate losses may be offset by another part of the law. That provision would require drugmakers to provide discounts to states for drugs sold to Medicaid managed care plans hired by the states. Yet even with those new discounts, some states project that they will see overall losses in the rebate programs
California, for instance, stands to lose $50 million next year alone because of the changes, according to Toby Douglas, the state's deputy Medicaid director. Douglas said that estimate was "very preliminary." He expects firmer numbers after the federal government provides more details about the change, which could come as soon as Wednesday.
Anne Murphy, Indiana's secretary of the Family and Social Services Administration, circulated a memo predicting losses of $400 million over 10 years because the federal government plans to "confiscate" a portion of its rebates. A spokesperson added that the estimate is based on state officials' reading of the law and that they are awaiting guidance, too.
The new law will increase the minimum rebates that drug firms must offer Medicaid programs from 15.1 percent to 23.1 percent for most brand name medications. Minimum rebates would also be increased for other drugs, including generics.
Under the old policy, states sent Washington a proportion equal to the share of Medicaid funding the federal government paid. The law says that the federal government now will get 100 percent of the rebate funding "attributable" to the increase from 15.1 to 23.1 percent. (Any rebates above 23.1 percent will still be shared.)
Industry analysts have suggested that wording may give the agency overseeing Medicaid some leeway in how it administers the rebate change to soften the impact on states.
The federal Medicaid agency refused to discuss the effects the provision could have on states. But, a spokeswoman said the agency would release guidelines "very soon."
State officials worry that since states already were getting rebates well above the previously required 15 percent, the change will cost nearly all of them millions of dollars a year. Based on 2009 Medicaid data, states received average rebates of 38.5 percent.
Officials "are very unhappy that their money is being taken away at a time when the states cannot afford this," said Ann Kohler, the director of the National Association of State Medicaid Directors.
As of December, 44 states had exceeded Medicaid spending projections for the fiscal year that ends Sept. 30, according to a survey released in February by the Kaiser Family Foundation. And at least 29 states had either recently made reductions in benefits and physician pay to their programs or expected to do so soon. (KHN is a project of the Kaiser Family Foundation.)
All but three states, Arizona, Massachusetts and New Mexico, would stand to lose money, in many cases millions of dollars a year, because of the drug rebate changes, according to a state-by-state examination of 2009 Medicaid spending records by Kaiser Health News. The 47 other states and the District of Columbia had negotiated average rebates from drugmakers that are better than required and in many cases far surpass the 23.1 percent requirement. For example, Georgia's rebates average about 50 percent.
The analysis compared total rebates received by federal and state governments with total drug spending for each state's Medicaid program for 2009, according to data from the federal agency that oversees Medicaid.
Drugmakers did not return calls asking for comment, and state officials were reluctant to discuss rebates, which are protected by confidentiality agreements with the firms.
One caveat in trying to determine a state's losses is that each state negotiates rebates on a drug-by-drug basis and lower rebates apply to generics and other classes of drugs.
Some state lawmakers are already calling on federal officials to back away from the proposal. "Some things may need to be changed," said Sharon Treat, a Democratic Maine legislator. "For those of us that have been working hard to get health care passed, it would be a slap in the face if we lose money."
Maine could face particularly steep losses under the change because the state does not use managed care for any of its Medicaid enrollees and would not benefit from the provision offering discounts for managed care programs.
Forty-one states use managed care plans to cover about 70 percent of Medicaid enrollees nationwide. However, only 16 of them depend on the managed care programs to administer drug benefits, while others have opted to pay for many drugs directly to get rebates. Those 16 states would have the most to gain from the new managed care policy.
The provision might encourage additional states to use managed care plans for drug coverage. That could lead to a reduction in drug spending and is raising concerns among some pharmaceutical makers.
Arizona is one of the states that will see a major benefit. It runs the entire Medicaid program through managed care plans, so the state did not benefit in the past from the federally required rebates. Because of the change, the program will likely gain significant new funding.
This story was produced through collaboration between NPR and Kaiser Health News(KHN), an editorially independent program of the Henry J. Kaiser Family Foundation, a nonpartisan health-care policy research organization. The Kaiser Family Foundation is not affiliated with Kaiser Permanente.
---------
"Exclusive: WellPoint routinely targets breast cancer patients"
By Murray Waas, April 22, 2010
LOS ANGELES (Reuters) – One after another, shortly after a diagnosis of breast cancer, each of the women learned that her health insurance had been canceled. First there was Yenny Hsu, who lived and worked in Los Angeles. Later, Robin Beaton, a registered nurse from Texas. And then, most recently, there was Patricia Relling, a successful art gallery owner and interior designer from Louisville, Kentucky.
None of the women knew about the others. But besides their similar narratives, they had something else in common: Their health insurance carriers were subsidiaries of WellPoint, which has 33.7 million policyholders -- more than any other health insurance company in the United States.
The women all paid their premiums on time. Before they fell ill, none had any problems with their insurance. Initially, they believed their policies had been canceled by mistake.
They had no idea that WellPoint was using a computer algorithm that automatically targeted them and every other policyholder recently diagnosed with breast cancer. The software triggered an immediate fraud investigation, as the company searched for some pretext to drop their policies, according to government regulators and investigators.
Once the women were singled out, they say, the insurer then canceled their policies based on either erroneous or flimsy information. WellPoint declined to comment on the women's specific cases without a signed waiver from them, citing privacy laws.
That tens of thousands of Americans lost their health insurance shortly after being diagnosed with life-threatening, expensive medical conditions has been well documented by law enforcement agencies, state regulators and a congressional committee. Insurance companies have used the practice, known as "rescission," for years. And a congressional committee last year said WellPoint was one of the worst offenders.
But WellPoint also has specifically targeted women with breast cancer for aggressive investigation with the intent to cancel their policies, federal investigators told Reuters. The revelation is especially striking for a company whose CEO and president, Angela Braly, has earned plaudits for how her company improved the medical care and treatment of other policyholders with breast cancer.
The disclosures come to light after a recent investigation by Reuters showed that another health insurance company, Assurant Health, similarly targeted HIV-positive policyholders for rescission. That company was ordered by courts to pay millions of dollars in settlements.
In his push for the health care bill, President Barack Obama said the legislation would end such industry practices. Making the case for reform in a September address to Congress, Obama specifically cited the cancellation of Robin Beaton's health insurance. Aides to the president, who requested they not be identified, told Reuters that no one in the White House knew WellPoint was systematically singling out breast cancer patients like her.
Many critics worry the new law will not lead to an end of these practices. Some state and federal regulators -- as well as investigators, congressional staffers and academic experts -- say the health care legislation lacks teeth, at least in terms of enforcement or regulatory powers to either stop or even substantially reduce rescission.
"People have this idea that someone is going to flip a switch and rescission and other bad insurance practices are going to end," says Peter Harbage, a former health care adviser to the Clinton administration. "Insurers will find ways to undermine the protections in the new law, just as they did with the old law. Enforcement is the key."
In a statement to Reuters, WellPoint said various specified criteria trigger rescission investigations, including certain types of medical claims. The company said it changed its rescission practices to ensure they are handled appropriately after a 2006 review of its policies prompted by public concern over rescission.
WellPoint also said it created a committee that includes a physician for making rescission decisions. The company also noted that it established a single point of contact for members undergoing an investigation and enacted an appeals process for applicants who disagree with the original determination.
During the recent legislative process for the reform law, however, lobbyists for WellPoint and other top insurance companies successfully fought proposed provisions of the legislation. In particular, they complained about rules that would have made it more difficult for the companies to fairly -- or unfairly -- cancel policyholders.
For example, an early version of the health care bill passed by the House of Representatives would have created a Federal Office of Health Insurance Oversight to monitor and regulate insurance practices like rescission. WellPoint lobbyists pressed for the proposed agency to not be included in the final bill signed into law by the president.
They also helped quash proposed provisions that would have required a third party review of its or any other insurance company's decision to cancel a customer's policy.
The new law does leave open the possibility of reform in this area, these sources say. The reason, they say, is that much of the new legislation is essentially a roadmap, with regulations to be decided later.
"The lack of specificity doesn't mean that nothing is going to be done," said a senior congressional staffer who has played a key role in the health reform debate, "The law grants HHS (the Department of Health and Human Services) the discretion to promulgate regulations. This is very much a work in progress."
Among other things, the staffer said, the White House could revisit proposing tough new regulations requiring third party review of policy cancellations.
Victoria Veltri, the general counsel of Connecticut's Office of Healthcare Advocate, a state agency that investigates complaints by policyholders, says she has seen the success of such a process in her home state. One company, Aetna, has voluntarily agreed to engage in the third party review, with what she described as favorable results.
"I haven't seen an Aetna case in our office since they went to the third party review process," she said. "It's a powerful tool to have a third set of eyes required before someone is rescinded."
For its part, WellPoint said it began offering third-party reviews in 2008.
A senior Obama administration official said he remained confident that mandatory third party reviews of rescissions is not entirely out of reach.
"It might take some wrangling with the insurance industry, some strong-arming, maybe even use of the presidential bully pulpit," he said on condition of anonymity.
INSURERS' ANATHEMA: BREAST CANCER AND PREGNANCY
The cancellation of her health insurance in June 2008 forced Robin Beaton to delay cancer surgery by five months. In that time, the tumor in her breast grew from 2 centimeters to 7 centimeters.
Two months before Beaton's policy was dropped, Patricia Relling also was diagnosed with breast cancer. Anthem Blue Cross of Kentucky, a WellPoint subsidiary, paid the bills for a double mastectomy and reconstructive surgery.
But the following January, after Relling suffered a life-threatening staph infection requiring two emergency surgeries in three days, Anthem balked and refused to pay more. They soon canceled her insurance entirely.
Unable to afford additional necessary surgeries for nearly 16 months, Relling ended up severely disabled and largely confined to her home. As a result of her crushing medical bills, the once well-to-do businesswoman is now dependent on food stamps.
"It's not like these companies don't like women because they are women," says Jeff Isaacs, the chief assistant Los Angeles City Attorney who runs the office's 300-lawyer criminal division. "But there are two things that really scare them and they are breast cancer and pregnancy. Breast cancer can really be a costly thing for them. Pregnancy is right up there too. Their worst-case scenario is that a child will be born with some disability and they will have to pay for that child's treatment over the course of a lifetime."
Isaacs is a former federal prosecutor who spent much of his time with the U.S. Justice Department investigating corporate wrongdoing. Among state and federal regulators, he is now considered one of the toughest and most experienced foes of the health insurance industry. He has hired retired FBI agents to investigate full-time the practices of WellPoint and its Anthem Blue Cross subsidiary in California.
Still, Isaacs feels outgunned: "The industry just has these tremendous financial, legal and political resources that others don't," he said. "In my own state, regulators are often afraid or unwilling to go up against them. It is hard to figure out what the future brings."
In July 2008, Isaacs' office sued Anthem Blue Cross, alleging that more than 6,000 people in the state of California had their insurance canceled due to its "illegal rescission practices." The litigation is ongoing.
Last February, the insurer agreed to pay a $1 million fine and an additional $14 million in restitution to alleged victims to settle another lawsuit. This one was brought against it by the California Department of Insurance, which said the company violated state laws by improperly rescinding the policies of 2,330 people.
A year earlier, Anthem Blue Cross agreed to pay a $10 million fine to settle similar charges brought by a second agency in the state, the California Department of Managed Health Care, alleging that WellPoint had illegally rescinded more than 1,100 policyholders.
Despite the settlements, WellPoint denies wrongdoing. In a statement for this story, the company said: "The settlements you referenced with the California regulators expressly denied any admission of wrongdoing on the part of the company; companies settle matters for a number of reasons."
As part of his investigation, Isaacs has sought information from WellPoint about its use of algorithms to single out women with breast cancer or who are pregnant. The company has fought him vigorously and so far largely kept information from him, Isaacs said.
But in response to an inquiry last year from the House Energy and Commerce Committee, which was investigating rescission, WellPoint said that it initiates a claims review every time policyholders receive medical treatment for certain conditions. The company listed diagnostic codes that could trigger investigations. One was for breast tumors.
During an audit of Anthem Blue Cross by the California Department of Managed Health Care, company employees showed regulators internal records revealing that pregnant women also automatically had their medical histories examined.
WellPoint says that even though the company routinely investigates policyholders with diseases such as breast cancer shortly after a diagnosis, it only cancels policies if it finds something wrong. It says the practice is necessary to keep down costs for other policyholders.
In testimony before the House committee last year, Brian Sassi, the president and CEO of WellPoint's consumer division, asserted: "I want to emphasize that rescission is about stopping fraud and material misrepresentation that contributes to spiraling health care costs. Rescission is a tool employed by WellPoint and other health insurers to protect the vast majority of policyholders who provide accurate and complete information from subsidizing the cost of those who do not."
But state regulators, congressional investigators and consumer advocates say that in only a tiny percentage of canceled health insurance cases was there a legitimate reason.
A 2007 investigation by the California Department of Managed Health Care bore this out. The agency randomly selected 90 instances in which Anthem Blue Cross of California dropped the insurance of policyholders after diagnoses with costly or life-threatening illnesses to determine how many were legally justified.
None were. "In all 90 files, there was no evidence (that Blue Cross), before rescinding coverage, investigated or established that the applicant's omission/misrepresentation was willful," the DMHC report said.
IN THE COMPANY OF WOMEN
Singling out women with breast cancer for aggressive investigation with the intent of canceling their insurance stands in stark contrast not only to the public image WellPoint cultivates for itself but also to the good work it does for many other policyholders with breast cancer.
WellPoint CEO Braly has taken a strong personal interest in women's health issues. Foremost among them is how to increase services to people with breast cancer.
The company prides itself on being one of the United States' largest corporations with women at the helm. Besides Braly, two high-powered, politically connected women sit on WellPoint's board: Susan Bayh, the wife of retiring Democratic Sen. Evan Bayh of Indiana, and Sheila Burke, who was chief of staff to former Senate Republican leader Bob Dole.
On Braly's initiative, WellPoint has funded groundbreaking studies about the disparities in quality of health care to minority women -- including women with breast cancer.
WellPoint has worked to encourage mammography for at-risk women. Personalized letters -- followed up by phone calls -- are sent to more than 80,000 women between the ages of 52 and 69 if they have not had a mammogram in the past year. The company conducts automated calls for women ages 40 to 69 to make sure they are getting mammograms.
Once diagnosed, WellPoint has set up an "Breast Cancer Resource Center" for its policyholders to help them "navigate the complex health care system."
And in May 2009, WellPoint's charitable foundation, the WellPoint Foundation LLC, provided a grant for the American Cancer Society for its "Hope Lodges," which allow cancer patients and family members free lodging and support while receiving care far from home. The grant funded Hope Lodges in Wisconsin, Ohio, Indiana and Kentucky, where Patricia Relling resides.
To Relling, charitable giving does not mitigate the harm done to her and other cancer patients who have had their health insurance canceled after a breast cancer diagnosis. "I can't pay for my medicine," she said. "I haven't been able pay for surgery that I need for two years. It doesn't make any sense."
Relling adds: "I laud people who give money to charity -- but not at the expense of cancer patients and people who have paid health insurance premiums for 20 years and never missed a payment -- and then get canceled when they most need their coverage. What about the thousands of people who have their policies canceled by their company for no good reason? When are they going to make that right?"
Why would WellPoint on the one hand work to improve health care for women with breast cancer while automatically investigating every single woman diagnosed with breast cancer for possible cancellation of their policies?
Karen L. Pollitz, a research professor at the Health Policy Institute at Georgetown University, offers one possible explanation: "It is important for these companies' profit margins that they get rid of policyholders with expensive diseases," she said. "If one company were to stop, it would no longer be competitive with the others. They argue they have to do this to stay in the game."
The investigation last year by the House Energy and Commerce Committee determined that WellPoint and two of the nation's other largest insurance companies -- UnitedHealth Group Inc and Assurant Health, part of Assurant Inc -- made at least $300 million by improperly rescinding more than 19,000 policyholders over one five-year period.
WellPoint itself profited by more than $128 million from the practice, and the committee suggested that the figure might be largely understated because the company refused to provide information about cancellations by several subsidiaries.
During the yearlong debate over health care reform, as the White House and Democrats in Congress savaged insurance industry practices, WellPoint took as much heat as any company. Among other things, it was slammed for trying to raise premiums by as much as 39 percent for some customers. One in nine of all Americans are policyholders with WellPoint or one of its subsidiaries.
Braly, who was named CEO of the Indianapolis-based company in February 2007, appeared before a U.S. congressional hearing two months ago and defended the rate hikes as reflecting higher medical costs.
PAYING THE PRICE
Losing her policy had serious consequences for Beaton, the retired Texas nurse. In June 2008, she learned that her insurance had been dropped just as she was about to undergo surgery for breast cancer. She had been recently diagnosed and told her cancer was a particularly aggressive type that would require a double mastectomy.
On the Friday before the Monday she was scheduled for surgery, Beaton's insurance company said it would not pay for the operation. It also informed her that it was launching an investigation of her medical history to see if she had misled the company and would sue if it found that to be the case.
Beaton's insurance problems stemmed from a visit to the dermatologist's office just before her breast cancer diagnosis. A word written on her chart was mistakenly determined to be precancerous, she said in testimony last year before the congressional committee. In fact, she was being treated for acne.
Even after her dermatologist told the insurer he indeed had only treated her for acne, her lack of insurance meant Beaton could not schedule her surgery.
Her doctors had told her that even the slightest delay might endanger her life, so Beaton was frantic. She contacted anyone who might be able to help her. As a nurse, she knew which charities and hospitals to plead her case. Still, she got nowhere until her congressman, Republican Representative Joe Barton, successfully took up her cause.
Five months elapsed between the time her surgery was originally scheduled and the time WellPoint agreed to pay for it. During that delay, the cancerous mass in her breast had more than tripled. She had to undergo a radical double mastectomy and her survival rate is a fraction of what it would have been had she been allowed to have the surgery earlier.
"Blue Cross and Blue Shield will do anything to get out of paying for cancer," Beaton said at the hearing.
After her surgery, Beaton joined a cancer support group. Four of the women in her group, she says, had their insurance canceled as a result of a cancer diagnosis. Two of the four subsequently had to declare bankruptcy because of staggering medical bills.
Earlier, in November 2006, WellPoint dropped the policy of another Texas woman -- shortly after she too was diagnosed with a cancerous lump in her breast, according to congressional investigators who have reviewed internal company records.
WellPoint told the Energy and Commerce Committee the cancellation of the woman's policy was justified because she had not told them that she had osteoporosis and bone density loss -- even though neither has anything to do with breast cancer and an insurance agent rather than the woman herself may have been responsible for those minor omissions.
Investigators for the committee stumbled upon the woman's case during their inquiry into rescission. But in the records that WellPoint produced, the woman's name and contact information was blacked out.
When the committee asked WellPoint for more information about her, the company refused to provide it, citing federal privacy laws for their policyholders.
Committee investigators said they then suggested WellPoint could itself inform the woman that a congressional committee had interest in her case. If the woman wished to talk to the committee, they suggested, she could contact it on her own.
WellPoint declined to do that as well, according to the committee records.
Stephen J. Northrop, WellPoint's vice president for federal affairs, wrote to Energy and Commerce Committee Chairman Henry A. Waxman, a California Democrat, explaining why the company could not comply:
"You asked that WellPoint send a letter to certain policyholders whose de-identified files WellPoint produced to the Committee earlier this year. The letter you would have proposed would explain that there is an ongoing Committee inquiry and would invite the policyholders to call a Congressional staff member who works for the committee.
"However, as WellPoint's outside counsel advised your staff by telephone yesterday, we are prohibited by the federal Health Insurance Portability and Accountability Act (HIPAA) from using our policyholders' protected health information for this purpose."
In a brief telephone interview with Reuters and later via email, Northrop declined to comment. In the email, Northrop said that a company spokesperson would answer further questions about his correspondence with the congressional committee, but the spokesperson did not address that particular matter.
In California, Yenny Hsu has a similar story to tell about WellPoint subsidiary Blue Cross Anthem. In a civil suit filed against the insurer in 2006, Hsu alleged her health insurance was rescinded shortly after a breast cancer diagnosis.
The pretext for canceling her insurance, the lawsuit alleged, is that Hsu failed to disclose having been exposed to Hepatitis B for a short time as a child. Her lawsuit has since been settled on undisclosed terms, her attorney, William Shernoff, said in an interview.
In Kentucky, Relling underwent her double mastectomy in April 2008. Anthem Blue Cross and Blue Shield of Kentucky footed the bill. Then in December of that year, she underwent reconstructive surgery, and Anthem paid once again.
The following month, however, her nightmare began.
DOWNWARD SPIRAL
Relling suffered a horrific staph infection caused by her stay in the hospital. She was rushed back there in the early morning of January 15 and was admitted shortly after 5:30 a.m.
The incision from her reconstructive breast surgery was reopened. Her abdomen was flushed with six full liters of antibiotic fluid until the incision was closed. Two days later, her condition worsened, requiring yet another emergency surgery.
This second surgery necessitated multiple blood transfusions simply to keep her alive. The infection was so severe her entire umbilicus, the interior of her belly button, had to be removed, as well as many abdominal muscles, because the infection had already eaten away most of it.
While recovering, Relling started having trouble with her insurance. Her medication after the surgery cost $4,446 a month. But Anthem would only pay for 10 days and then no more, she recalled in an interview.
Luckily, one doctor gave her free samples and another found a dispensary where could obtain the medication at a reduced price. But other days she would go without.
In June 2009, she was informed that her insurance was being canceled -- just before she was about to undergo another reconstructive surgery, which she was forced to postpone. She has now gone 16 months without the necessary surgery.
As a result, she is severely disabled. The pain and discomfort often only allows her to be able to stand for 20 or 30 minutes a day, sometimes even less.
Reconstructive surgery might help her to become mobile again and perhaps go back to work full-time. She once enjoyed successful careers as an art gallery owner, interior decorator, and as a writer. She had plenty of money, drove a Mercedes and traveled the world on whim. Not anymore.
Today she is on food stamps. She has taken her Social Security early, which means that when she is older, she will be eligible for fewer benefits. She buys clothes from consignment stores she once donated to. She recently got some part-time work as a copywriter, which she can do from home, but that barely pays for her drug prescriptions, let alone surgery.
She spends her days calling pharmaceutical companies because many now have programs to assist indigent customers.
Relling waits hours to be seen by a doctor at a clinic, if she can be seen at all. "The thing I didn't understand about going poor is that your time no longer has value to others," she says.
She seeks out religious charities to pay the rent. "Some have rules that they will only give to people who belong to that church or of their faith."
One charity she contacted after being informed that it provides financial assistance to breast cancer patients told her that it does so only for women of color and of a certain age. "This is my full time job now. You go around and around and around," she says, her voice trailing her off.
Technically, rescission was not the reason Relling lost her health insurance, according to correspondences with the company she provided to Reuters. Rather, it was canceled because she did not answer letters from her insurance company requesting information about her employment history.
Relling says the letter was sent to an address which she hadn't lived at it for some time, and she never even saw it until recently. When she brought this information to WellPoint's attention, she said, the company ignored her.
"Rescission is just one method to get rid of someone or no longer provide them coverage," says Isaacs, the deputy Los Angeles City Attorney. "They can say forms are not filled out properly; they will just find any pretext."
Congressional investigators for the House Energy and Commerce Committee who have investigated Relling's claim say they have concluded that WellPoint improperly canceled her insurance. The company declined to comment at all on her case, saying that client confidentiality precludes them from doing so, although Relling says she welcomes the company to talk publicly about the matter.
On her living room table still sits correspondence with her former insurance company.
Deb Moessner, the company's president and general manager, wrote Relling last July 13: "Ms. Relling, please know that is never pleasant to deliver unfavorable news to our members. However, there are situations that occur, such as yours, that leave us with no alternatives. Because you or your agent did not provide this vital information, your ... health coverage terminated effective July 1, 2009."
In the letter, Moessner added: "Please know that we wish you the best in regaining the healthy lifestyle you described prior to your recent illnesses."
(Additional reporting by Lewis Krauskopf; editing by Jim Impoco and Doina Chiacu)
---------
"Nearly 4M people could pay without health coverage"
By Stephen Ohlemacher, AP, April 22, 2010
WASHINGTON – Nearly 4 million Americans — the vast majority of them middle class — will have to pay a penalty if they don't get insurance when President Barack Obama's health care overhaul law kicks in, according to congressional estimates released Thursday.
The penalties will average a little more than $1,000 apiece in 2016, the Congressional Budget Office said in a report.
Most of the people paying the fine will be middle class as Obama's comprehensive law is phased in over the next few years. In his 2008 campaign for the White House, Obama pledged not to raise taxes on individuals making less than $200,000 a year and couples making less than $250,000.
Republicans have criticized the requirement that Americans get coverage, even though the idea was originally proposed by the GOP in the 1990s and is part of the Massachusetts health care plan signed into law in 2006 by then Gov. Mitt Romney, a Republican. Attorneys general in more than a dozen states are working to challenge it in federal court as unconstitutional.
"The individual mandate tax will fall hardest on Americans who can least afford to pay it, many of whom were promised subsidies by the Democrats and who the president has promised would not pay higher taxes," said Rep. Dave Camp of Michigan, the top Republican on the tax-writing House Ways and Means Committee.
Sen. Chuck Grassley of Iowa, the top Republican on the Senate Finance Committee, said while Obama and congressional Democrats celebrate the benefits of the law, they have an obligation to acknowledge the flip side. "There's a price for not participating, and people will pay it," Grassley said.
Democrats argue that the requirement and the penalties are a necessary part of a massive overhaul designed to expand coverage to millions who now lack it. They point out that getting more Americans, especially young and healthy people, in the insurance pool will reduce costs for others and could lower premiums.
"The new law will make health insurance affordable for everyone and CBO's analysis confirms that the vast majority of uninsured Americans will find health care affordable and choose to participate," said White House spokesman Nick Papas.
Americans who don't get qualified health insurance will be required to pay penalties starting in 2014, unless they are exempt because of low income, religious beliefs, or because they are members of American Indian tribes. The penalties will be fully phased in by 2016.
About 21 million nonelderly residents will be uninsured in 2016, according to projections by the CBO and the Joint Committee on Taxation. Most of those people will be exempt from the penalties.
Under the new law, the penalties will be phased in starting in 2014. By 2016, those who must get insurance but don't will be fined $695 or 2.5 percent of their household income, whichever is greater.
After 2016, the penalties will be increased by annual cost-of-living adjustments. People will not be required to get coverage if the cheapest plan available costs more than 8 percent of their income.
The penalties will be collected by the Internal Revenue Service through tax returns. However, the IRS will not have the authority to bring criminal charges or file liens against those who don't pay.
About 3 million of those required to pay fines in 2016 will have incomes below $59,000 for individuals and $120,000 for families of four, according to the CBO projections. The other 900,000 people who must pay the fine will have higher incomes.
The government will collect about $4 billion a year in fines from 2017 through 2019, according to the report.
---------
"The challenges of implementing health care reform"
By Charles Joffe-Halpern, The North Adams Transcript, Op-Ed, April 23, 2010
It has been said the only thing harder than passing health legislation is actually implementing health legislation. Given the complexity of the recently passed health care law, along with the emotionally-charged resistance coming from health reform's opponents, the challenge of implementation has only begun.
Two thoughtful observers of the challenges of implementation are Dr. Atul Gawande, the Boston-based surgeon who has written extensively on health policy, and Drew Altman, president of the Kaiser Family Foundation.
Writing in The New Yorker, Gawande reminds us that the passage of Medicare in 1965, brought about similar strong resistance. He notes: "The American Medical Association had waged war to try to stop the program, and doctors weren't about to abandon the fight against "socialized medicine" simply because it had passed into law. The Ohio Medical Association, with 10,000 physician members, declared that it would boycott Medicare, and a nationwide movement began. Race proved an even more explosive issue. Many hospitals, especially in the South, were segregated, and the law required them to integrate in order to receive Medicare dollars."
In the end, though, the AMA finally gave up the fight after President Johnson gave it a role implementing the rule and regulations of the program, and the resisting hospitals decided to abandon segregation rather than lose federal dollars.
The attacks now come from party politics, rather than the medical profession. Dealing with this resistance could be more challenging because, while Medicare was implemented two years after the legislation was passed, the major benefits of health reform now -- the coverage expansions, subsidies and insurance market reforms -- do not start until 2014.
Altman, in a piece titled "Implementation is Forever," suggests we have a number of important tasks before us. These include "establishing the facts about what the law does and does not do, providing detailed information to the public about how different groups will be affected by the law, and helping people take advantage of the benefits it provides."
While direction and support will ultimately come from Washington, it will fall on each community to educate its residents and to implement health reform. To paraphrase the late Tip O'Neill, "All health care is local."
With this in mind, it is important to know that, under health reform, there are benefits being implemented this year that could immediately help area small businesses. Starting this year, businesses with fewer than 25 full-time equivalent employees with average salaries of less than $50,000 a year, could be eligible for tax credits that will pay up to 35 percent of the employer's health insurance costs (25 percent for non-profit organizations). To receive the tax credit, employers have to pay for 50 percent of the cost of the premiums. The tax credit will increase to 50 percent in 2014. The current legislation will allow businesses to receive the tax credits for two years after 2014.
Another important benefit for area residents will go into effect this September, when health insurers will be required to permit adult children to stay on family policies until age 26. This applies to all plans, unless the adult child has an offer of coverage through his or her employer. Some insurance companies have begun allowing young adults to stay on their parents plan already. Both married and unmarried dependents qualify for this dependent coverage.
Another immediate benefit is the $250 reimbursement Medicare beneficiaries could receive who fall into the "doughnut-hole" of the Medicare part-D drug program. For a concise list of all of the benefits, go to www.healthreform.gov.
The health reform law is multi-faceted and will affect individuals of all age groups and all of the major health care stakeholders. Altman recognizes that in the coming years, as the many provisions of the law are implemented, the impact of the health care law on access, cost and care will need to be monitored closely, but he cautions:
"Experience in every other developed nation teaches us that reforming health care is not like fixing a problem with your car. You don't find the problem, identify a solution, and then it is fixed. After passing their form of comprehensive national health reform legislation, every other nation continued to make corrections and improvements and to struggle with the tension between ever more expensive medical care and limited resources."
Atul Gawande's and Drew Altman's observation will be valuable, as our own version of national health reform evolves over the coming years.
-
Charles "Chip" Joffe-Halpern is the executive director of Ecu-Heath Care and the president of the board of directors of Health Care for All in Boston. He can be contacted at cjoffehalpern@nbhealth.org.
-
---------
-

-
FILE - In this April 1, 2010 file photo, President Barack Obama speaks about health care reform during an event at the Portland Expo Center, in Portland, Maine. Many experts believe the health care overhaul law falls short on taming costs, and that will force Congress to revisit health care in a few years. (AP Photo/Alex Brandon, File)
-
"Health care law's unfinished business: cost curbs: In time, Congress could be forced to revisit health care overhaul to find more savings"
By Ricardo Alonso-Zaldivar, Associated Press Writer, April 25, 2010
WASHINGTON (AP) -- What's it going to cost me?
That's the single biggest unanswered question about President Barack Obama's new health care overhaul law -- and its weak spot.
Many experts believe the law falls short on taming costs, and that will force Congress to revisit health care in a few years.
While it seems hard to believe now, Republicans might want to participate in a debate over costs, perhaps opening the way for limits on malpractice lawsuits and other ideas they've advocated.
"Now that the baseline question of coverage has been answered, it would be irresponsible if we didn't come back and try to do more on costs," said Sen. Mark Warner, D-Va., who voted for the bill and led efforts to squeeze more savings.
"I think there is going to be a debate in the Republican Party on whether they should waste all their energy on repeal or make an effort to do something on cost containment," Warner said.
For now, the political parties are too polarized -- and lawmakers too exhausted -- to contemplate health care 2.0. Conservatives are planning court challenges, and some Republican leaders hold out the promise of repeal. But economic reality probably will bring lawmakers back to the table.
Insurance premiums are likely to keep going up over the next few years. Experts predict that the law's early benefits -- such as expanded coverage for children and young adults -- could nudge rates a little higher than would otherwise have been the case. Also, insurers and medical providers could try to raise their prices ahead of big shifts set for 2014.
Under the 10-year, $1 trillion plan, 2014 is when competitive insurance markets for individuals and small businesses are expected to open, and tax credits start flowing to help millions of middle-class households now uninsured. Medicaid will expand and pick up millions of low-income people. Most Americans would be required to carry health insurance, except in cases of financial hardship. Insurers no longer could turn away those in poor health.
More than 30 million previously uninsured people would gain coverage quickly -- and they'll start going to the doctor for care previously postponed. Increased demand will push up health care spending, putting more pressure on premiums.
The cost controls in the bill are unlikely to provide much of a counterweight. Democrats scrambling to line up votes for the final bill weakened a provision that would have enforced austerity through a hefty tax on high-cost employer coverage.
Other savings in the law -- mainly Medicare cuts -- may prove politically unsustainable, according to the government's own experts.
The problem isn't that the 2,700-page law is devoid of ideas for curbing costs. Many mainstream proposals are incorporated in some form. But what will work?
While the law creates a commission to keep pursuing deeper Medicare savings, there's no overall cost control strategy and no single official to coordinate many experiments seeking greater efficiency.
"This bill takes a sort of spaghetti approach to cost control," said MIT economist Jonathan Gruber, who supports the broad goals of the overhaul. "You throw a bunch of stuff against the wall and see what will stick. Health care, Round Two, is when we will make a serious effort at cutting costs down, based on what this law has shown us."
If the law gets a B plus for expanding coverage to 95 percent of eligible Americans, it probably deserves a C minus or D for cost control. The U.S. spends $2.5 trillion a year on health care, with some results worse than what other developed countries get by spending far less.
"Most people who have problems with health care costs now are not going to see much change in the next few years," said Mark McClellan, who ran Medicare under former Republican President George W. Bush. "Hopefully some of these ideas will work, but it's not automatic. I do hope we can revisit this in a more bipartisan manner."
A look at some of the law's main cost control provisions:
--INSURANCE MARKET
Starting in 2014, the overhaul sets up new state-level insurance supermarkets called exchanges, intended to enable small businesses and individuals buying their own coverage to pool purchasing power. In theory, that would inject competition into markets now dominated by one or two major insurers in most states.
It also would reduce insurers' overhead by giving them access to many customers in one place. The companies would be heavily regulated by state and federal authorities, and proposed premium increases would get a close look.
"Individuals and small businesses will, over time, have something much more predictable to look at," said Christine Ferguson, former Massachusetts public health commissioner under Republican Gov. Mitt Romney. "We will have much more predictable rates of growth in health care costs."
Romney, a potential GOP presidential candidate in 2012, signed a similar law in Massachusetts, but is now calling for repeal of the federal version.
--PAYMENT REFORMS
Using Medicare as the lab, the law includes experiments designed to change the way medical providers are paid. It encourages them to keep patients healthier by avoiding foreseeable complications.
Doctors and hospitals could band together to better coordinate care. Instead of paying piecemeal for visits and tests, providers would get a lump sum for managing patients with certain health conditions. Primary care providers would be encouraged to create "medical homes" for their patients, serving as wellness coaches and medical gatekeepers.
Successful experiments would be adopted as national policy.
--MEDICARE BOARD
The law sets up a board to hunt for Medicare savings. Congress could reject the proposals, but it wouldn't be able to tinker with them.
--INSURANCE TAX
Employer-sponsored health insurance is part of total compensation, but traditionally it's been tax-free.
The law imposes a 40 percent tax on health insurance plans worth more than $27,500 for a family plan, $10,200 for individual coverage. (Family coverage now averages $13,375.)
That could have been a firm nudge to get people into more frugal coverage. But facing stiff opposition from labor unions, Obama and congressional Democrats punted, postponing the effective date until 2018. That's after the president leaves office, assuming he's re-elected.
---------
"Uncertainty over Medicare pay sets doctors on edge"
By Ricardo Alonso-zaldivar, Associated Press Writer, May 27, 2010
WASHINGTON – For the third time this year, Congress is scrambling to stave off a hefty pay cut to doctors treating Medicare patients — even as the Obama administration mails out a glossy brochure to reassure seniors the health care program is on solid ground.
The 21.3 percent cut will take effect June 1 unless lawmakers intervene in the next few days. Recurring uncertainty over Medicare fees is making doctors take a hard look at their participation in a program considered a bedrock of middle-class retirement security.
If the problem is allowed to fester, it could undermine key goals of President Barack Obama's health care overhaul, which envisions using Medicare to test ideas for improving the quality of care for all Americans. Doubts about Medicare's stability can also create political problems for Democrats in the fall elections, since polls show seniors are worried about the impact of the remake on their own care.
"We will not have that cut," vowed House Speaker Nancy Pelosi, D-Calif.
How lawmakers will resolve the problem is unclear. Initially, Democrats had talked about a five-year fix, then three years. Now leaders are proposing postponement through the end of 2011.
"It is disappointing that Congress is considering shorter temporary action at the 11th hour," said James Rohack, president of the American Medical Association. "The current payment system is fatally flawed, and delaying solving the problem will make it bigger and harder to handle."
Abolishing the cuts altogether — as the AMA wants — would be expensive, an estimated $200 billion or more over 10 years. But doctors say they've had it with temporary reprieves that don't eliminate the underlying threat.
"In the past two years, (lawmakers) keep coming up to the deadline — or a little past it — and waiving the cuts for shorter and shorter periods of time, which makes us uneasy," said Dr. Susan Crittenden, a primary care physician practicing near Raleigh, N.C.
"The current uncertainty about what the fee schedule will be, and whether at some point there will be a 20 percent cut, makes it harder to accept new Medicare patients," Crittenden said.
Although government surveys indicate that Medicare beneficiaries' access compares favorably to that of privately insured patients, doctors and patients say that's not always the case.
Crittenden's practice takes very few new Medicare patients, since the program pays her medical group well below private insurers' rates. "I like to take care of older adults, but I have rent to pay, and a staff to pay," she explained.
Some longtime Medicare advocates fault Congress and the Obama administration for not dealing with the doctor cuts during the marathon health care overhaul debate. That would have pushed the cost of the legislation above the $1 trillion, 10-year limit Obama set.
Economist Marilyn Moon, a former Medicare trustee, said the health care legislation's $500 billion in cuts to hospitals, insurers and other Medicare providers should have been earmarked to deal with doctor fees first, with anything left over used to help the uninsured.
"They should have used Medicare dollars to fix this," said Moon, who helped oversee program finances from 1995-2000. "It's irresponsible" that the health care law left such a major issue unresolved, she said, while at the same time claiming to reduce the federal deficit.
"I think we should have put a crowbar in our wallets and still come up with the money for the uninsured," added Moon. "But in trying to meet a range of goals — having the bill not be more than $1 trillion and having it be budget-neutral — they dumped this issue." Moon now directs the health care program at the American Institutes for Research.
The problem with doctor fees stems from requirements of a 1990s deficit reduction law. Well before Obama was elected president, Congress had settled into a pattern of routinely waiving the cuts. But that only compounded the long-range problem, increasing the size of future cuts required to meet savings targets.
The Obama administration supports repealing the cuts altogether, and the House passed legislation to do that. But a Senate version couldn't muster the 60 votes needed to move forward.
"The key problem is that no one wants to pay for it," said John Rother, top strategist for AARP, the seniors' lobby. "This is something that requires some additional revenue, and we should face up to that fact."
Meanwhile, the Obama administration is mailing out a brochure to explain the benefits of the new health care law to 46 million Medicare recipients. The law, says the brochure, "keeps Medicare strong and solvent." Republicans are calling it political spin.
---------
"Taking insurers to task"
The Berkshire Eagle, Editorial, June 24, 2010
A major weakness in the much-compromised federal health care reform law passed three months ago is that it did not give the federal government the power to regulate premiums. Washington can attack premiums indirectly, but the best weapon the president has against greedy insurers is the bully pulpit, which President Obama employed Tuesday in the face of evidence that insurers are dramatically and not unexpectedly hiking premiums on Americans without real justification.
David Axelrod, the president's senior adviser, said Tuesday that executives of leading health insurers gathered in the East Room were warned not to use the new law as an excuse for "rate gouging." Also in attendance at the meeting were state insurance commissioners who have the authority to work with Washington to assure consumers that they are not being gouged by insurers.
The president acknowledged that there are many reasons why health insurance rates would climb, among them rate increase requests from hospitals that put considerable pressure on insurers. These demands, made largely by large, big-city hospitals with considerable leverage, are a component of health care reform that is yet to be adequately addressed. However, a report released Monday by Health Care for America Now, a coalition that backs the new law, put the onus for premium increases primarily on the insurance companies by revealing that while premiums skyrocketed 97 percent over the past eight years, medical inflation reached a comparatively modest 37 percent.
Happily, many states are taking the initiative against unreasonable insurance requests, beginning with Massachusetts. After insurers ignored his admonition not to unilaterally raise premiums dramatically, Governor Patrick shocked them by exercising the authority his office has long had but had never used to deny nine of the 10 rate requests. California, New York and Pennsylvania are now taking steps to block punishingly large premium hikes.
Both the Congressional Joint Committee on Taxation and the nonpartisan Congressional Budget Office project that the law will have a minimal effect on premiums, largely because of government subsidies. Insurers predict otherwise, and their recent increases smell like self-fulfilling prophecies designed to undermine the law and give ammunition to critics. Obamacare will soon benefit Americans by preventing insurers from refusing to cover children with pre-existing conditions or dropping coverage because the policyholder made the mistake of becoming ill -- these provisions will be in place within three months. The fight to keep premiums low will be even harder, but it can be won if the states also adopt the cause.
---------
"Medicaid cuts: teeth pulled, transplant called off"
By Carla K. Johnson, AP Medical Writer, December 13, 2010
CHICAGO – In Illinois, a pharmacist closes his business because of late Medicaid payments. In Arizona, a young father's liver transplant is canceled because Medicaid suddenly won't pay for it. In California, dentists pull teeth that could be saved because Medicaid doesn't pay for root canals.
Across the country, state lawmakers have taken harsh actions to try to rein in the budget-busting costs of the health care program that serves 58 million poor and disabled Americans. Some states have cut payments to doctors, paid bills late and trimmed benefits such as insulin pumps, obesity surgery and hospice care.
Lawmakers are bracing for more work when they reconvene in January. Some states face multibillion-dollar deficits. Federal stimulus money for Medicaid is soon to evaporate. And Medicaid enrollment has never been higher because of job losses.
In the view of some lawmakers, Medicaid has become a monster, and it's eating the budget. In Illinois, Medicaid sucks up more money than elementary, secondary and higher education combined.
"Medicaid is such a large, complicated part of our budget problem, that to get our hands around it is very difficult. It's that big. It's that bad," said Illinois Sen. Dale Righter, a Republican and co-chairman of a bipartisan panel to reform Medicaid in Illinois, where nearly 30 percent of total spending goes to the program.
Medicaid costs are shared by the federal and state governments. It's not just the poor and disabled who benefit. Wealthier people do, too, such as when middle-class families with elderly parents in nursing homes are relieved of financial pressure after Medicaid starts picking up the bills.
Contrary to stereotype, it's the elderly and disabled who cost nearly 70 cents of every Medicaid dollar, not the single mother and her children.
In California, Medicaid no longer pays for many adult dental services. But it still pays for extractions, that is, tooth-pulling. The unintended consequence: Medicaid patients tell dentists to pull teeth that could be saved.
"The roots are fine. The tooth could be saved with a root canal," said Dr. Nagaraj Murthy, who practices in Compton, Calif. "I had a patient yesterday. I said we could do a root canal. He said, `No, it's hurting. Go ahead and pull it. I don't have the money.'"
Murthy recently pulled an elderly woman's last tooth, but Medicaid no longer pays for dentures.
"Elderly patients suffer the most," Murthy said. "They're walking around with no teeth."
States can decide which optional services Medicaid covers, and dental care is among cutbacks in some places. Last year's economic stimulus package increased the federal share of Medicaid money temporarily. But that money runs out at the end of June, when the federal government will go back to paying half the costs rather than 60 to 70 percent. So more cuts could be ahead.
During the Great Recession, millions of people relied on the Medicaid safety net. Between 2007 and 2009, the number of uninsured Americans grew by more than 5 million as workers lost jobs with employer-based insurance. Another 7 million signed up for Medicaid.
Just when caseloads hit their highest point, the nation's new health care law required states not to change the rules on who's eligible for Medicaid. That means states can't roll up the welcome mat by tightening Medicaid's income requirements.
So states have resorted to a variety of painful options.
In Arizona, lawmakers stopped paying for some kinds of transplants, including livers for people with hepatitis C. When the cuts took effect Oct. 1, Medicaid patient Francisco Felix, who needs a liver, suddenly had to raise $500,000 to get a transplant.
The 32-year-old's case took a dramatic turn in November when a friend's wife died, and her liver became available. Felix was prepped for surgery in hopes financial donations would come in. When the money didn't materialize, the liver went to someone else, and Felix went home. His doctor told him he has a year before he'll be too sick for a transplant.
"They are taking away his opportunity to live," said his wife, Flor Felix. "It's impossible for us or any family to get that much money." The family is collecting donations through a website and plans a yard sale this weekend, she said.
The choices are difficult for states that have already cut payments to doctors and hospitals to the bone.
"If we don't see an economic recovery where state revenues rebound, they're really going to be very strained on how they can make ends meet," said Diane Rowland, executive director of the Kaiser Commission on Medicaid and the Uninsured.
States may consider lowering payment rates to nursing homes or home health agencies or further reducing payments to doctors, Rowland said.
"The problem here is the program is pretty lean, and payment rates are pretty low," she said. Patients can't find care because fewer doctors accept the low payments.
Prescription drug coverage in states is an optional benefit, another possible place to cut, Rowland said. "But if you cut back on people's psychotropic drugs, is that penny-wise and pound-foolish? Do they end up in institutions where Medicaid pays more for their care?"
In Illinois, late payments became the rule.
Tom Miller closed his pharmacy in rural southern Illinois this summer and is going through bankruptcy, largely because the state was chronically late making Medicaid payments to him. Most of his former customers are in the program.
With the state sometimes months behind in payments, he couldn't pay his suppliers. Five workers lost their jobs when his business closed.
"You can only fight it for so long," said Miller, 54. He now works as a pharmacist in a hospital. He misses his old clients, the families he grew to know.
"I was in my third generation. I've had moms who had kids. I saw the kids raised, and they had their own children," he said. As a neighborhood pharmacist, "you're their friend. You're family."
---------
"Gov't: Health tab to hit $4.6 trillion in 2020"
By RICARDO ALONSO-ZALDIVAR - Associated Press | AP – July 28, 2011
WASHINGTON (AP) — The nation's health care tab is on track to hit $4.6 trillion in 2020, accounting for about $1 of every $5 in the economy, government number crunchers estimate in a report released Thursday.
How much is that? Including government and private money, health care spending in 2020 will average $13,710 for every man, woman and child, says Medicare's Office of the Actuary.
Compare it to this year, when U.S. health care spending is projected to top $2.7 trillion, about $8,650 per capita, or roughly $1 of $6 in the economy. Most of those dollars go to provide care for the sickest people.
Along with rising costs, the report found that the share of the health care tab paid by the government keeps growing, approaching half the total.
The update from Medicare economists and statisticians is an annual barometer of a trend that many experts say is unsustainable, but doesn't seem to be slowing. A political compromise over the nation's debt and deficits might succeed in tapping the brakes on health care, but polarized lawmakers have been unable to deliver a deal.
The analysis found that President Barack Obama's health care overhaul would only be a modest contributor to growing costs, even though an additional 30 million otherwise uninsured people stand to gain coverage.
Instead, health care spending keeps growing faster than the economy because of high cost of medical innovations and an aging society that consumes increasing levels of service.
Many of the newly insured people under the health care law will be younger and healthier, so they cost less. Over a million young adults under age 26 have already gained coverage through their parents' insurance. Millions more will get insurance when the law's big coverage expansion kicks off in 2014.
That year, health care spending will jump by 8 percent. But over the 2010-2020 period covered by the estimate, the average yearly growth in spending will be only 0.1 percentage point higher than without Obama's overhaul. Most of the newly insured are not expected to require much pricey hospital care, generally needing only doctor visits and prescription drugs.
Another reason for the optimistic prognosis is that cuts and cost controls in the health care law start to bite down late in the decade. However, the same nonpartisan Medicare experts who produced Thursday's estimate have previously questioned whether that austerity will be politically sustainable. If hospitals and other providers start going out of business, Congress may reverse the cuts.
The report found that health care spending in 2010 grew at a historically low rate of 3.9 percent, partly because of the sluggish economy. That will change as the economy shakes off the lingering effects of the recession.
Government, already the dominant player because of Medicare and Medicaid, will become even more important. By 2020, federal, state and local government health care spending will account for just under half the total tab, up from 45 percent currently. As the health care law's coverage expansion takes effect, "health care financing is anticipated to further shift toward governments," the report said.
Estimates from previous years had projected that the government share would already be at the 50 percent mark, but the actuary's office changed its method for making the complex calculations. Under the previous approach, some private payments such as worker's compensation insurance had been counted in the government column.
Technical accuracy — not political pressure — was behind that change, said one of the experts who works on the estimates. "This was an internal decision that was not influenced by any outside party," said Stephen Heffler.
Separately, another new report finds that the United States continues to spend far more on health care than other economically developed countries. The study by the Commonwealth Fund found that U.S. health care spending per person in 2008 was more than double the median — or midpoint— for other leading economies. Although survival rates for some cancers were higher in the U.S., the report found that quality of care overall was not markedly better.
The Medicare actuary's report on health care spending is published in the journal Health Affairs. The actuary's office is responsible for long-range cost estimates.
___
On the Internet:
Health Affairs: www.healthaffairs.org
---------
"Survey: Health insurance costs surge in 2011"
Survey: 2011 employer-sponsored health insurance costs surge, breaking moderate growth trend
Tom Murphy, AP Business Writer, September 27, 2011
INDIANAPOLIS (AP) -- The cost of employer-sponsored health insurance surged this year, snapping a trend toward moderate growth, but experts say these increases may slow again in 2012.
Annual premiums for family coverage climbed 9 percent and surpassed $15,000 for the first time, according to a report released Tuesday by the Kaiser Family Foundation and the Health Research and Educational Trust. Premiums for single coverage rose 8 percent compared to 2010.
That compares to increases last year of 3 and 5 percent for family and single coverage, respectively. The study shows that premiums for both family and single coverage have more than doubled since 2001, while worker wages have risen 34 percent.
Kaiser CEO Drew Altman said a number of factors may have played a role in this year's percentage jump. He noted that health care costs continue to rise, and insurer profits and the health care overhaul also have some impact.
The overhaul, which Congress passed last year, aims to eventually cover millions of uninsured people. Kaiser said initial provisions of the law contributed between 1 and 2 percentage points to this year's premium hikes, which is about what many insurance analysts and benefits experts expected.
Companies and workers split premiums for employer-sponsored coverage, the most common form of health insurance in the United States, and employers generally pick up 70 percent of the bill or more.
Businesses likely reacted to these cost increases by giving a smaller raise or no wage increase to their workers, said Helen Darling, CEO of the National Business Group on Health, a nonprofit organization that represents large employers on health care issues.
"(Workers) basically are giving their pay raise to the health system," said Darling, who was not involved with the Kaiser study. "It's really bad news."
The annual study was conducted earlier this year and includes results from more than 2,000 companies nationwide. It also indicates that many more families than previously believed have benefited from a popular provision in the overhaul that allows young adults to stay on a parent's health plan until they turn 26.
Kaiser asked employers how many people were added to their insurance plans because of this provision and estimated that 2.3 million young adults enrolled. Last week the government had reported that the number of uninsured young adults had dropped by nearly 1 million since the law took effect, a finding independently corroborated by Gallup.
The difference isn't necessarily a contradiction.
The Kaiser survey may have counted young adults who were covered by a more expensive policy and switched to their parent's plan to save money.
Many workers are about to receive notices from their employers regarding health insurance coverage for next year. Altman said he cannot say whether this year's increase represents a bad omen for 2012 or if it is just a one-year blip.
Insurers have been saying for months that health care use is growing more slowly this year, something industry observers pin on a sluggish economy. Altman and other benefits experts say that could lead to lower premium increases next year, since insurers base their rates in part on how often people use care.
Benefits consultant Mercer said earlier this month an employer survey it did shows that 2012 health insurance costs will rise by the smallest amount since 1997.
The Kaiser survey shows a steady increase in companies offering high-deductible plans, which come with lower premiums but make consumers pay more out of pocket for care. This insurance is often paired with health savings accounts that let people save pretax for medical expenses.
Altman said he expects that trend to continue growing as employers try to control premiums.
"This is the main tool that employers have in the toolbox right now, so we're going to see more and more high-deductible plans with bigger and bigger deductibles," he said.
Associated Press writer Ricardo Alonso-Zaldivar contributed to this report from Washington, D.C.
---------

FILE - In this Aug. 14, 1935, file photo President Franklin Roosevelt signs the Social Security Bill in Washington. In 1935 Americans struggle to pay for medical care amid the Great Depression. Roosevelt favors creating national health insurance, but decides to push for Social Security first. He never gets the health program passed. But his Social Security bill will provide old age pensions and unemployment insurance. From left are: Chairman Doughton of the House Ways and Means Committee; Sen. Wagner, D-N.Y, co-author of the bill, Secretary Perkins, Chairman Harrison of the Senate Finance Committee, Rep. Lewis, D-Md., co-author of the measure. (AP Photo/File)
"America's health care reform through history"
By Connie Cass, Associated Press, March 24, 2012
The three days of arguments beginning before the Supreme Court on Monday may mark a turning point in a century of debate over what role the government should play in helping all Americans afford medical care. A look at the issue through the years:
1912: Former President Theodore Roosevelt champions national health insurance as he tries to ride his progressive Bull Moose Party back to the White House. It's an idea ahead of its time; health insurance is a rarity and medical fees are relatively low because doctors cannot do much for most patients. But medical breakthroughs are beginning to revolutionize hospitals and drive up costs. Roosevelt loses the race.
1929: Baylor Hospital in Texas originates group health insurance. Dallas teachers pay 50 cents a month to cover up to 21 days of hospital care per year. The plan grows into Blue Cross.
1932: After five years of work, doctors, economists and hospital administrators on the independent Committee on the Costs of Medical Care publish their report about the increasing costs of health care and the number of people going untreated. They say health care should be available to all.
1935: Americans struggle to pay for medical care amid the Great Depression. President Franklin D. Roosevelt favors creating national health insurance, but decides to push for Social Security first. He never gets the health program passed.
1942: Roosevelt establishes wage and price controls as part of the nation's emergency response to World War II. Businesses can't attract workers with higher pay so instead they compete through added benefits, including health insurance, which unexpectedly grows into a workplace perk. Workplace plans get a boost the following year when the government says it won't tax employers' contributions to employee health insurance.
1945: Saying medical care is a right of all Americans, President Harry Truman calls on Congress to create a national insurance program for those who pay voluntary fees. The American Medical Association denounces the idea as "socialized medicine." Truman tries for years but can't get it passed.
1960: John F. Kennedy makes health care a major campaign issue but as president can't get a plan for the elderly through Congress.
1965: Medicare for people age 65 and older and Medicaid for the poor signed into law. President Lyndon B. Johnson's legendary arm-twisting and a Congress dominated by his fellow Democrats succeeded in creating the kind of landmark health care programs that eluded his predecessors.
1971: Sen. Edward M. Kennedy, D-Mass., offers his proposal for a government-run plan to be financed through payroll taxes.
1974: President Richard Nixon puts forth a plan to cover all Americans through private insurers. Employers would be required to cover their workers and federal subsidies would help others buy insurance. The Watergate scandal intervenes.
1976: Jimmy Carter pushes a mandatory national health plan, but a deep economic recession helps push it aside.
1986: Congress passes and President Ronald Reagan signs into law COBRA, a requirement that employers let former workers stay on the company health care plan for 18 months after leaving a job, with the worker bearing the cost.
1988: Congress expands Medicare by adding a prescription drug benefit and catastrophic care coverage. It doesn't last long. Barraged by protests from older people upset about paying a tax to finance the additional coverage, Congress repeals the law the next year.
1992: Helping the uninsured becomes a big issue of the Democratic primaries and spills over into the general election. Democrat Bill Clinton wants to require businesses to provide insurance to their employees, with the government helping everyone else; Republican President George H.W. Bush proposes tax breaks to make it easier to afford insurance.
1993: Newly elected, Clinton puts first lady Hillary Rodham Clinton in charge of developing what becomes a 1,300-page plan for universal coverage. It requires businesses to cover their workers and mandates that everyone have insurance. The plan meets strong Republican opposition, divides congressional Democrats and comes under a firestorm of lobbying from businesses and the health care industry. It never gets to a vote in the Democrat-led Senate.
2003: President George W. Bush persuades Congress to add prescription drug coverage to Medicare in a major expansion of Johnson's "Great Society" program for seniors.
2008: Hillary Rodham Clinton makes a sweeping health care plan, including a requirement that everyone have coverage, central to her bid for the Democratic presidential nomination. She loses to Barack Obama, who promotes his own less comprehensive plan.
2009: Obama and the Democratic-controlled Congress spend an intense year ironing out a compromise that requires companies other than very small businesses to cover their workers, mandates that everyone have insurance or pay a fine, requires insurance companies to accept all comers, regardless of any pre-existing conditions, and assists people who can't afford insurance.
2010: Congress passes the Patient Protection and Affordable Care Act, designed to extend health care coverage to more than 30 million uninsured people. Obama signs it into law March 23.
---------
"Obama ex-advisers want to put $2.8T health care industry on a budget to keep costs manageable"
By Associated Press, The Washington Post, September 2, 2012
WASHINGTON — Some of President Barack Obama’s former advisers are proposing major changes aimed at controlling health care costs as political uncertainty hovers over his health law.
Call it Health Care Overhaul, Version 2.0. Their biggest idea is a first-ever budget for the nation’s $2.8-trillion health care system, through negotiated limits on public and private spending in each state.
The approach broadly resembles a Massachusetts law signed this summer by Democratic Gov. Deval Patrick that puts pressure on hospitals, insurers, and other major players to keep rising costs within manageable limits. It could become the Democratic counterpoint to private market strategies favored by Republican presidential nominee Mitt Romney and running mate Paul Ryan.
Health costs lie at the heart of budget problems confronting the next president. Health care accounts for 18 percent of the economy and about one-fourth of the federal budget, and many experts believe it can’t grow unchecked without harming other priorities. Because the United States spends much more than other advanced countries, there’s a consensus that savings from cutting waste and duplication won’t harm quality.
“We think of these as the next generation of ideas,” said Neera Tanden, who was a senior member of the White House team that helped pass the health law. Tanden is now president of the Center for American Progress, a Washington think tank close to the administration.
Under the proposal, the major public and private players in each state would negotiate payment rates with service providers such as hospitals. The idea is to get away from paying for each individual test and procedure. Negotiated rates could be based on an entire course of treatment. Payments would have to fit within an overall budget that could grow no faster than the average rise in wages.
The spending limits would be enforced by an independent council, but crucial details need to be spelled out. In Massachusetts, for example, budget-busting providers will be required to file plans with the state laying out how they’ll amend their spendthrift ways.
The federal government would provide grants to states interested in developing their plans.
Tanden joined a brain trust of former administration officials floating the proposal recently in the New England Journal of Medicine. The group included Peter Orszag (former budget director), John Podesta (transition director), Donald Berwick (first Medicare chief), Ezekiel Emanuel (Orszag’s health policy guru), and Joshua Sharfstein (former No. 2 at the Food and Drug Administration). Also on board was former Senate Majority Leader Tom Daschle, D-S.D., Obama’s first pick to shepherd his health care overhaul.
Their proposal includes other ideas, such as a malpractice liability shield for doctors who follow best clinical practices, and competitive bidding for all Medicare supplies and lab tests, not just home health equipment. All of the signers support Obama’s health care law, but see cost control as unfinished business.
Republicans are already scoffing at the budgeting proposal.
“Politically, it is really tone deaf,” said economist Douglas Holtz-Eakin, president of the American Action Forum, a free-market think tank. “There is no way Americans are going to trust any government entity to say how much the nation should spend on (health care). It is at odds with our values and our history and has zero chance of happening.”
But neither party has a monopoly on trust when it comes to changing health care.
A recent Kaiser Family Foundation poll found that 55 percent of Republicans would prefer to keep Medicare the way it is instead of nudging future retirees toward private insurance plans, as Romney and Ryan propose.
Republican leaders generally want to reshape the health care system along the lines of the changes that 401(k) plans have brought to pensions. Instead of open-ended benefits, individuals would get a fixed payment for health insurance and pick coverage from private plans competing to drive down costs and improve quality.
Republicans also believe government has no business telling private individuals and employers how much they can budget for health care.
“The aim of public policy should not be to stop people spending their own money on their health care,” said Stuart Butler, a top health policy expert with the conservative Heritage Foundation. (While the new Massachusetts plan limits what public programs spend, it does not require private payers to do the same.)
Tanden, the former White House aide, says she thinks budgets and negotiated payments will be less threatening and more politically acceptable than giving people a voucher-like payment and sending them into the marketplace. Medicare would share in the benefit if costs can be checked for the country as a whole.
“We think of this as the answer to ‘premium support’,” said Tanden, referring to the term Republicans prefer for the Romney-Ryan Medicare plan. “What this is really enabling is a private sector negotiation. Under premium support what will happen is consumers will pay more.”
In Massachusetts, the new cost control law has its share of skeptics, but it doesn’t seem to have provoked a backlash.
“These global budgets are going to be negotiated between health insurers and providers,” said Jay Gonzalez, the state’s secretary of administration and finance. “They are agreeing to pay for services in a different way. It isn’t rationing. It isn’t capping.”
Massachusetts enacted its original health care overhaul under then-Gov. Romney in 2006, expanding coverage to an estimated 98 percent of state residents. Obama’s law covering the uninsured could still be repealed if Romney wins the White House. The main cost controls in the president’s plan — a board to restrain Medicare spending and a tax on high-cost private health insurance — wouldn’t start to bite for another few years.
The White House has had little to say about the new ideas from Obama’s former advisers. That could change if Obama is re-elected and plunges into budget negotiations with Congress.
---------
Jon Hurst & Bill Vernon: “'Non-profit' care providers crushing small business”
By Jon Hurst & Bill Vernon, Op-Ed, The Berkshire Eagle, March 29, 2017
BOSTON — Small businesses are the backbone of the Massachusetts economic engine. But many are under increasing economic pressure as they try to keep their doors open. Small businesses have two ways to stay in business: increase sales or lower their operating costs. But under a global economy where consumers can buy goods and services worldwide, increasing sales is becoming more difficult. This means that small business owners must lower operating expenses, including payroll and benefits in order to compete and succeed.
On the other hand, highly profitable "non-profit" health care providers in Boston have a different economy and operate under their own rules. Health care providers are important and valuable institutions in our community. But consumers of health care, who drive in from the suburbs to visit a Boston emergency room for a sprained ankle have no idea what their health care costs are or the difference in costs between a Boston based provider or a community provider.
Often the consumer faces no immediate economic impact since the costs are covered by their insurance. The impact is only felt when everyone's premiums increase. For small businesses paying between 50 percent and 90 percent of their employees' premiums, the result is double digit premium increases annually. With no ability to lower such costs, the viability of these companies become endangered thereby forcing them to cut jobs.
There is consensus that small businesses are paying too much for their health care. Regardless, some hospitals argue that they need higher payments from the private sector because they lose money on government-subsidized patients. Yet publicly available data refutes that claim.
Boston entitlement
Experts know from years of government reports that market power drives certain hospitals' bottom lines. They have little incentive to operate efficiently, or to lower their costs. They live under their rules where there is no competition, nor incentive to bring prices and costs down for small businesses and consumers. To the contrary, these providers continue to operate under the premise that higher costs and higher salaries is a "community benefit" that consumers must continue to subsidize in order to support their charitable mission.
This entitled mentality predates RomneyCare and ObamaCare. In fact, certain Boston hospitals have received millions in subsidies through a combination of earmarked taxpayer dollars, supplemental payments, uncompensated care funding and hidden assessments on employers. These subsidies continue despite the fact that 97 percent of the population of Massachusetts is now insured under the ACA. Curiously, billions of dollars of old and new funding sources are available for these hospitals to spend, without any reforms or accountability to force them to implement cost controls or efficiencies. We seem to reward these providers for charging us higher prices!
To make matters worse, some of these same providers are advocating for a new $600 million tax on employers. A $2,000 per employee tax would hammer small employers who are struggling with premiums far higher than what the rest of the country pays. Not only would this tax help to further enhance their bottom lines, it also shows a lack of desire on their part to manage their costs, as well as a lack of concern for the economic future of small businesses in our state.
Many employers who offer good, quality health insurance would unfortunately also be forced to pay hefty fines under this tax proposal. Add tens of thousands of dollars in health care tax payments on top of existing premiums and many will face the decision of either dropping coverage or closing for good.
It's time for our elected leaders to push for cost efficiency among hospitals and physician groups so that we as small businesses consumers have relief from escalating health care costs. They would also help state and local government budgets that are also feeling the similar pressure from increasing health care costs. It's time that we have a health care system where our health care premiums and out-of-pocket costs are predictable and affordable; where providers compete based on the quality and cost of the care they provide; and a system where employees of small businesses are not forced to unfairly subsidize providers through premiums and taxes.
Consumers and taxpayers share a common interest and would benefit from transparency in pricing, lower costs and premiums, as well as the choice to use health care providers where they live. It's time for government to infuse competition and cost efficiencies among health care providers and payers — like small business owners — bring us better value, not higher premiums and out of pocket costs.
Jon Hurst is president of the Retailers Association of Massachusetts. Bill Vernon is state director of the National Federation of Independent Business.
---------
1/15/2019
There is a bill in the U.S. House of Representatives, H.R.676, "The Expanded and Improved Medicare for All Act," which has a growing number of sponsors. Is Congresswoman Annie Kuster a sponsor of H.R. 676? Does Congresswoman Annie Kuster support "The Expanded and Improved Medicare for All Act"? Please support this current legislation that would create a federal government single payer healthcare insurance system that covers all U.S. Citizens. Thank you for your time and consideration.
- Jonathan Melle
---------
Opinion: "Long-term care should be covered by Medicare. Until then, here are actions we can take" By Josefina Carbonell, Yahoo! News, March 12, 2022
We are getting older, we are getting sicker and we need more help.
Our older population has been steadily increasing. Did you know that people over 65 are predicted to overtake children under 18 in population size by 2034?
But we have health issues. According to the Centers for Disease Control and Prevention, 85% of older adults have at least one chronic health condition and 60% have at least two chronic conditions. These conditions range from arthritis to cancer, diabetes to asthma.
Many older Americans need help not only with chronic conditions, but with the activities of daily life, such as bathing, dressing and eating. In fact, there’s a 70% chance that someone turning 65 today will need long-term care services and supports. And 20% of us will need it for longer than five years.
The first place we turn to for help as we get older are our family members. Families provide 80% of all the long-term care in this country, and comprise the largest segment of our caregiver workforce. But the growing need for medical long-term care coupled with overworked and unpaid caregivers means that paid care, by professionals and paraprofessionals, is also a crucial part of the equation.
Costs are high
But how do you pay for it?
Don’t count on the government to help, unless you have dire financial need and can qualify for Medicaid, which covers basic long-term care. If you’re part of the majority of us over 65 covered by Medicare or Medicare Advantage plans, you’re out of luck. They only cover short-term hospital or nursing home stays due to injury.
And have you looked at the cost for long-term care lately? If not, buckle up, because this is going to be a bumpy ride.
In 2020, the monthly cost to stay in a private room in a nursing home, or one that provides nursing care, help with daily living activities, and the availability of 24-hour medical care, averages almost $8,821 per month. Compare that to the average social security check of $1,555, and you can see that you need a whole lot of savings to cover the balance, even for the most diligent savers among us.
What about long-term care insurance, you might ask. Well, you may be one of the 7.5 million Americans who have long-term care insurance, according to the American Association for Long-Term Care Insurance. That’s only 14% of the US population of people 65 and older who have coverage.
The bottom line: Unless you are wealthy (self-pay), have paid long-term care insurance or are destitute, you won’t be able to afford care.
While I’d love to see long-term nursing home care coverage in Medicare and Medicare Advantage plans, the dollars needed for that may take years to get.
In the meantime, here are some other actions we can take.
Could government help?
The first is to provide more governmental support for family member caregivers.
Today, there are a variety of Medicaid-funded programs to pay in-home caregivers who are also family members. These vary by state, but include Medicaid Self-Directed Services, for those over age 60 who need help at home and are capable of directing the caregiving process, as well as live-in caregivers.
Yet there are no programs that provide financial assistance to family members caring for loved ones on Medicare or Medicare Advantage. I recommend that we ask the government to add self-directed and live-in caregiver support to the services offered by Medicare and Medicare Advantage.
I would also like to see more funding for the National Family Caregiver Support Program, part of the Older Americans Act. It doesn’t provide compensation to family members who are caregivers, but does pay outside caregivers to provide respite care, or occasional care, when family caregivers need a break.
My second suggestion is to provide more education and support around the prevention of chronic conditions for older Americans.
We need to work on getting the message across that we need to get healthier earlier in life – exercising a little bit more, eating the right foods and taking care of ourselves. That means we need to have better access to healthcare to manage our chronic conditions and be healthier as we achieve old age. Those who are most at-risk for chronic conditions are those who are poor or illiterate, so it makes sense to focus on those communities.
In the short term, a combination of education to manage and prevent chronic conditions as well as support for family caregivers will help the financial crisis of older Americans who need long-term care. Ultimately, the U.S. needs a long-term care policy that will help all older Americans in need.
Josefina Carbonell is the senior vice president of Long-Term Care at Independent Living Systems. She was assistant secretary for aging in the U.S. Department of Health and Human Services under President George W. Bush.
---------
Letter: "Close the loophole keeping breast cancer patients from the health care they qualify for"
By Denise Smith | The Salt Lake Tribune: The Public Forum | March 10, 2024
Lawmakers have enormous power to impact our daily lives. Our representatives in Washington have the opportunity to make a difference for thousands of Utahns — by closing an arbitrary loophole keeping breast cancer patients from the healthcare they qualify for.
This year, an estimated 42,250 women and 530 men in the U.S. will die of breast cancer. Almost all these deaths — 90% — are because of metastatic disease: cancer that has spread from the breast to the bones, lungs, or other parts of the body. There is no cure.
I have metastatic breast cancer. I lost my mother to metastatic breast cancer at a young age, and also lost my cousin, Tarina, to the disease last year. I know first-hand how this disease impacts families.
Individuals who have metastatic breast cancer and can no longer work are entitled to Medicare coverage under Social Security Disability Insurance (SSDI); however, these patients must endure lengthy and arbitrary waiting periods for access to health care. With an average life expectancy of only three years for metastatic breast care patients, there is no time to waste.
This must change. That is why we, as advocates with the National Breast Cancer Coalition, want to see The Metastatic Breast Cancer Access to Care Act (H.R. 549, S. 663) enacted into law. This bill would waive the waiting periods and provide immediate access to those who already qualify. After all, they paid for it.
The legislation has strong bipartisan support in Congress, but Sens. Mitt Romney and Mike Lee have yet to support it. I urge them to do so immediately.
My cousin Tarina and her family would have benefited from this legislation, which would have granted her care she was already qualified to receive. Instead, she was forced to work up until just days before she entered hospice, just so she could afford insurance to pay for her medication.
Congress has the power to eliminate the barriers to health care and financial support for those with metastatic breast cancer. Now they need the will.
Denise Smith, Utah Advocate, National Breast Cancer Coalition, Lehi
https://www.stopbreastcancer.org/
----------












































































































































.png)
































































































































































































































































No comments:
Post a Comment